
Although often confused, andropause and adrenal fatigue are not the same. Andropause refers to the gradual decrease in testosterone production that occurs naturally in men as they age. Adrenal fatigue describes a theory suggesting that chronic stress weakens the adrenal glands, causing tiredness and low energy. But this concept is not supported by clinical research. The two share overlapping symptoms, but their causes and medical validity differ greatly.
What Is Andropause and Adrenal Fatigue?
Andropause (Male Menopause)
Andropause, sometimes called male menopause, comes from “andro,” which means male, and “pause,” which means to slow down. It describes a gradual drop in testosterone levels over time. This process involves the brain and the testes. These parts work together to control male hormone production.
Adrenal Fatigue
Adrenal fatigue is a term used to describe a proposed effect of long-term stress levels on the body in both men and women's health. The name comes from the adrenal glands. Adrenal glands release cortisol and help regulate the body’s stress response.
However, research shows this is not a formal medical diagnosis. Studies do not support the idea that the adrenal glands become “fatigued” or stop working in this way, and this does not reflect reduced adrenal function in healthy individuals
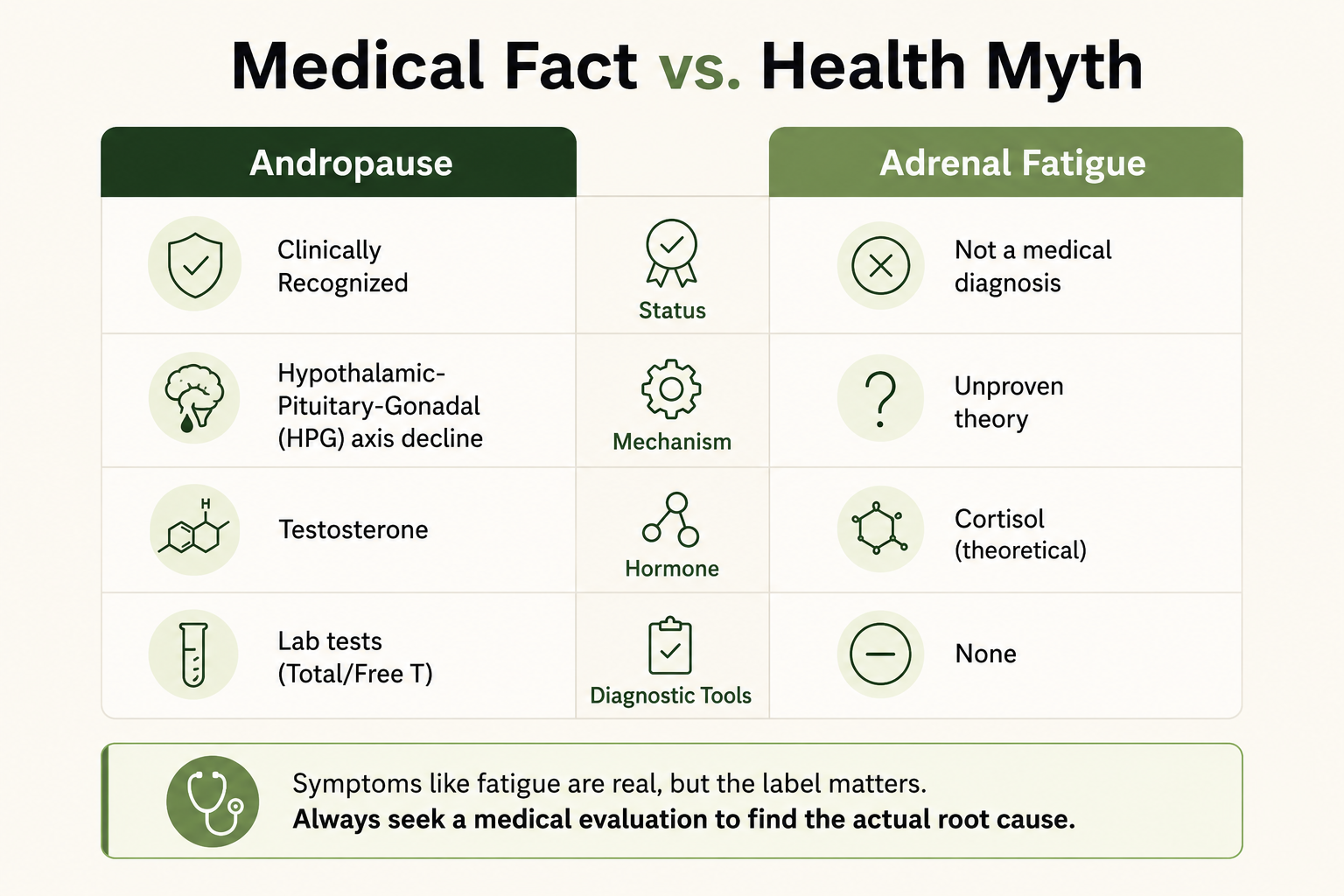
| Feature | Andropause | Adrenal Fatigue |
| Medical recognition | Yes | No |
| Hormone involved | Testosterone | Cortisol (theoretical) |
| Diagnosis | Lab tests + symptoms | Not recognized |
| Evidence | Strong clinical evidence | Unsupported by medical research |
Andropause vs Adrenal Fatigue: How the Body Systems Work
How Andropause Works
Andropause involves the brain and testes. The hypothalamus and pituitary gland send signals to the testes to make testosterone. Over time, these signals may weaken. This can lower hormone levels and affect the following:
- Sex drive
- Muscle mass leads to muscle loss
- Mood
- Energy
- Body fat and weight gain
How the Adrenal System Works
The adrenal glands sit above the kidneys and produce adrenal hormones such as cortisol, a key stress hormone.
These hormones help regulate:
- blood pressure
- Energy use
- Sleep cycles
- Stress response
- Immune balance
Cortisol plays a key role in how the body responds to stress. Changes in cortisol levels may affect these processes.
How These Conditions Happen
Andropause
According to the European Male Aging Study published in the New England Journal of Medicine, declining testosterone in aging men is linked not only to age, but also obesity, chronic illness, and metabolic conditions such as insulin resistance. This decline in testosterone production is a gradual process. Sleep loss may also contribute, as research in JAMA found reduced testosterone after short sleep duration.
Is Adrenal Fatigue Real? Understanding the Stress Response
Chronic stress can affect the body’s HPA axis and alter cortisol rhythms, according to endocrine research. However, a systematic review found no evidence that adrenal glands simply become “fatigued” or stop working from stress alone. So this condition still remains a myth.
Low Testosterone vs Stress Symptoms: Shared and Different Signs
Shared Physical Symptoms Include
- Fatigue
- Low motivation
- Poor focus or brain fog
- Difficulty falling asleep and sleep patterns
- Reduced sex drive
Common Andropause Symptoms
- Low libido
- Erectile dysfunction
- Loss of strength
- Belly fat gain
- Lower testosterone levels
More Common With Stress-Related Adrenal Symptoms
- Feeling tired or persistent fatigue
- Poor stress tolerance
- Mood swings
- Sleep disruption
Why Symptoms Alone Can Mislead: Look for the Root Cause
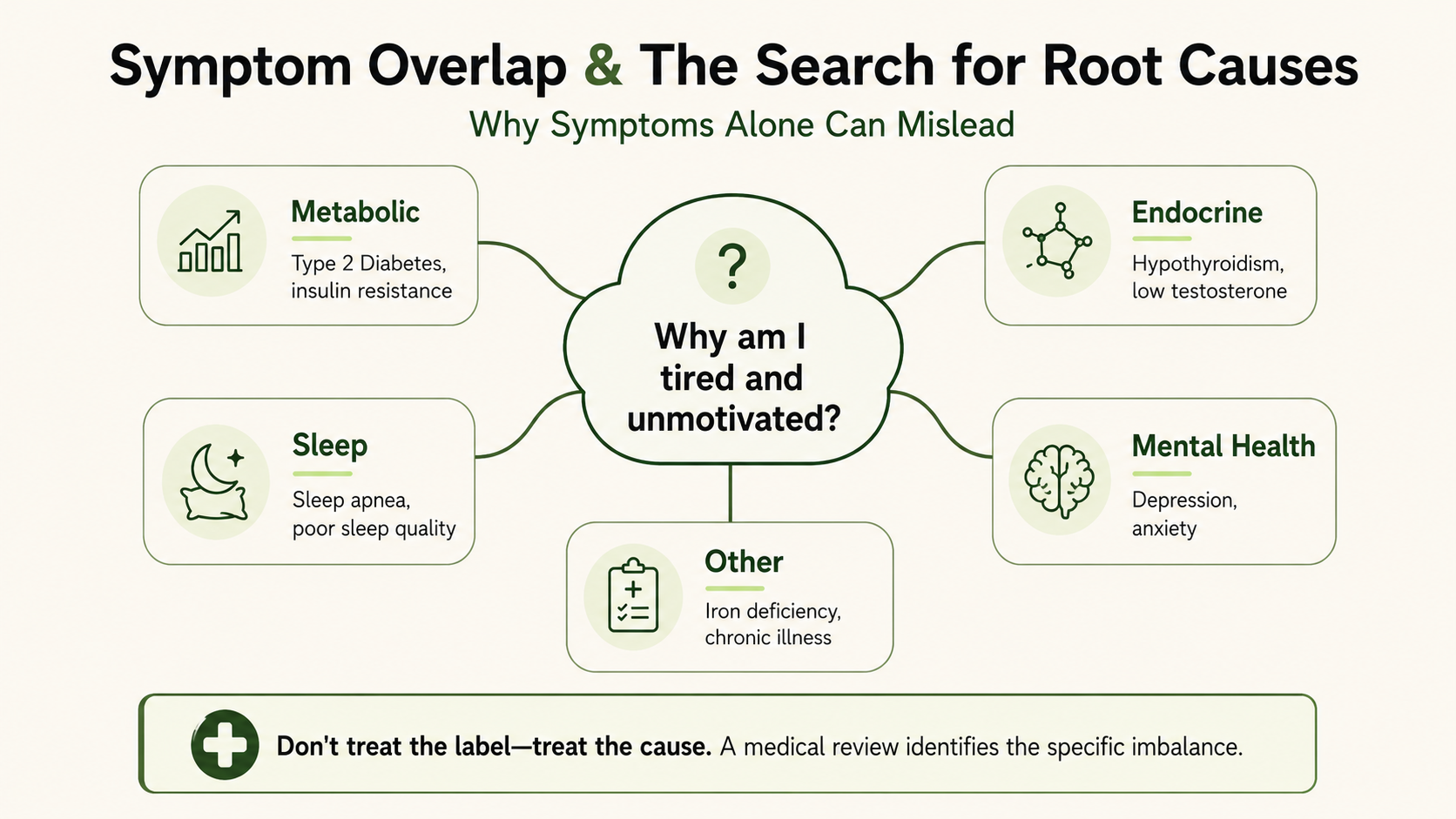
Many physical symptoms blamed on andropause and adrenal fatigue are nonspecific. Research shows fatigue, low libido, sleep problems, and mood changes often come from multiple conditions, including thyroid gland dysfunction, metabolic issues, or depression. This means the symptom label may only describe the surface problem, not the real disease underneath.
Conditions That Can Mimic Andropause
Low energy or low libido may also be linked to:
- Obesity
- Type 2 diabetes
- Sleep apnea
- Depression
- Medication effects
- Thyroid disorders
- Alcohol overuse
Studies show obesity and chronic illness can lower testosterone levels, sometimes reversibly. In these cases, treating the root cause may improve other hormones without direct testosterone therapy.
Conditions That Can Mimic “Adrenal Fatigue”
Fatigue and stress intolerance may also be linked to the following:
- Anxiety disorders
- Depression
- Burnout
- Chronic sleep loss
- Iron deficiency
- Thyroid disorders (including overactive thyroid gland or underactive thyroid)
- True adrenal insufficiency (rare but serious)
Systematic reviews found no evidence for adrenal fatigue as a medical diagnosis. This suggests many people labeled with adrenal fatigue may have another treatable hormone health condition.
Why Proper Testing Matters
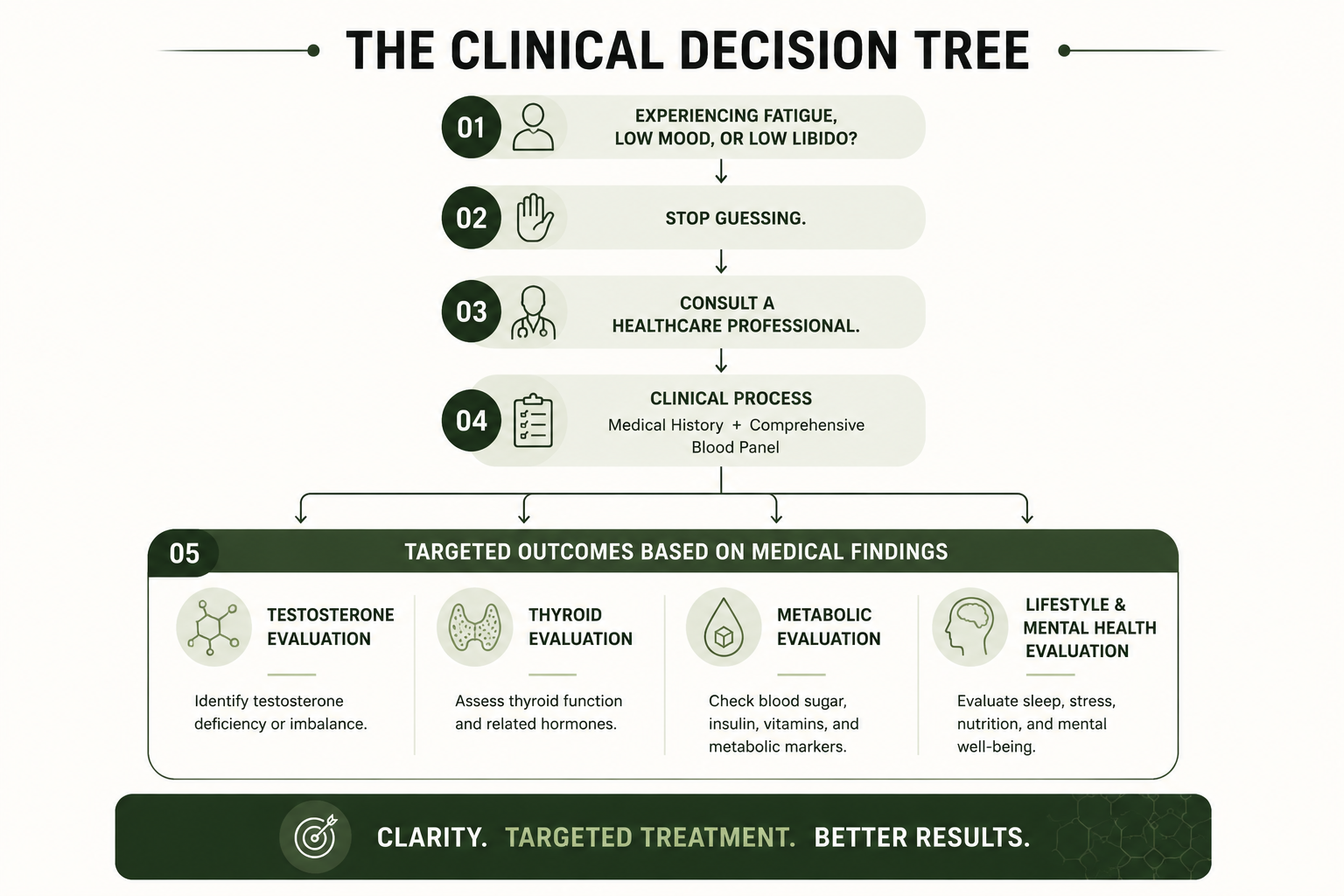
Published guidelines recommend using symptoms plus labs, history, and examination rather than symptom labels alone. This helps avoid missed diagnoses and unnecessary treatment.
Clinical Approaches for Andropause and Adrenal Fatigue Symptoms
When Andropause Is Clinically Evaluated
If symptoms and lab results (including free testosterone measurements) confirm low testosterone levels or testosterone deficiency, treatment options may include:
- Testosterone replacement therapy under medical supervision
- Bioidentical hormone replacement therapy as an alternative option
- Regular monitoring of free testosterone and other hormone levels
- Periodic blood pressure and cholesterol checks during treatment
The goal is to restore testosterone levels to a healthy range while monitoring for any side effects.
For those with suspected thyroid issues, testing thyroid hormone levels is essential before assuming symptoms are from andropause or adrenal fatigue.
Medical Treatment for True Adrenal Disorders
Adrenal fatigue is not a recognized medical diagnosis, and there is no specific treatment for it.
If testing shows a true adrenal health condition, such as adrenal insufficiency, care may include medicines like hydrocortisone or fludrocortisone under medical supervision. This applies only to confirmed disease, not to adrenal fatigue.
Natural Ways to Reduce Symptoms
Lifestyle Support for Hormone Optimization
Research suggests these steps may improve energy levels and hormonal health:
- Strength training
- Weight management
- Sleep improvement
- Stress management
- Balanced nutrition or Balanced diet
Areas With Limited Evidence
Some supplements are sold for adrenal support. Evidence is limited or mixed.
FAQs
Can fatigue mean low testosterone?
Sometimes. But fatigue may also come from sleep loss, depression, thyroid disease, or diabetes.
Is adrenal fatigue masking another illness?
It can be. Many symptoms linked to adrenal fatigue overlap with other conditions.
Can weight loss improve testosterone levels?
Research suggests weight loss may improve testosterone levels in some men with obesity.
What is the best next step if I have these symptoms?
A full medical review with labs is often more useful than self-diagnosis.
Can adrenal fatigue happen in both men and women?
Yes. The symptoms linked to adrenal fatigue can affect both men and women. However, it is not a recognized medical diagnosis, such symptoms should be checked for other causes.
How Is Hormonal Imbalance Diagnosed?
Proper testing includes measuring testosterone, cortisol, thyroid hormones, and other markers to identify hormonal imbalance.
Conclusion
Andropause and adrenal fatigue are often grouped together because they share similar symptoms. However, they are not the same. Andropause is linked to changes in testosterone levels, while adrenal fatigue is not a confirmed medical condition.
Many of these symptoms do not come from one cause. They may be linked to sleep problems, stress, metabolic health, or a hormone imbalance. This is why symptoms alone are not enough to make a diagnosis.
A clear and careful evaluation is important. Looking at the full picture helps identify the real cause and supports better decisions based on evidence.
References
Wu FC, Tajar A, Pye SR, et al. Identification of late-onset hypogonadism in middle-aged and elderly men. N Engl J Med. 2010 Jul;363(2):123–135. doi: 10.1056/NEJMoa0911101. PMID: 20554979. https://pubmed.ncbi.nlm.nih.gov/20554979/
Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018 May;103(5):1715–1744. doi: 10.1210/jc.2018-00229. PMID: 29562364. https://pubmed.ncbi.nlm.nih.gov/29562364/
Leproult R, Van Cauter E. Effect of 1 week of sleep restriction on testosterone levels in young healthy men. JAMA. 2011 Jun 1;305(21):2173–2174. doi: 10.1001/jama.2011.710. PMID: 21367988. https://pmc.ncbi.nlm.nih.gov/articles/PMC4445839/
Charmandari E, Tsigos C, Chrousos G. Endocrinology of the stress response. Annu Rev Physiol. 2005;67:259–284. doi: 10.1146/annurev.physiol.67.040403.120816. PMID: 15709959. https://pubmed.ncbi.nlm.nih.gov/15709959/
Cadegiani FA, Kater CE. Adrenal fatigue does not exist: a systematic review. BMC Endocr Disord. 2016 Aug;16:48. doi: 10.1186/s12902-016-0128-4. PMID: 27557747. https://pubmed.ncbi.nlm.nih.gov/27557747/
Viau V. Functional cross-talk between the hypothalamic-pituitary-gonadal and adrenal axes. J Neuroendocrinol. 2002 Jun;14(6):506–513. doi: 10.1046/j.1365-2826.2002.00798.x. PMID: 12047726. https://pubmed.ncbi.nlm.nih.gov/12047726/
Rosmond R. Stress-induced disturbances of the HPA axis. Eur J Endocrinol. 2005 Nov;153(1):1–11. doi: 10.1530/eje.1.01961. PMID: 15994739. https://pubmed.ncbi.nlm.nih.gov/12601304/
Corona G, Rastrelli G, Monami M, et al. Body weight loss reverts obesity-associated hypogonadotropic hypogonadism: a systematic review and meta-analysis. Eur J Endocrinol. 2013 Jun;168(6):829–843. doi: 10.1530/EJE-12-0955. PMID: 23482592. https://pubmed.ncbi.nlm.nih.gov/23482592/
Grossmann M. Low testosterone in men with type 2 diabetes: significance and treatment. J Clin Endocrinol Metab. 2011 Aug;96(8):2341–2353. doi: 10.1210/jc.2011-0118. PMID: 21632481. https://pubmed.ncbi.nlm.nih.gov/31616498/
Fernandez CJ, Chacko EC, Pappachan JM. Male obesity-related secondary hypogonadism: pathophysiology, clinical implications and management. Eur Endocrinol. 2019;15(2):83–90. doi: 10.17925/EE.2019.15.2.83. PMID: 31616498. https://pubmed.ncbi.nlm.nih.gov/31616498/



