Injections offer cost-effective, adjustable dosing but may cause mood and energy fluctuations due to peak-and-trough hormone levels. Pellets provide stable, long-term hormone release without the need for weekly needles, though they are more expensive, require a minor procedure for insertion, and cannot be adjusted once implanted. Both methods effectively treat low testosterone, so the best choice depends on your lifestyle, budget, and preference for either flexibility or consistency.
What Are Testosterone Pellets and Testosterone Injections?
If you are researching testosterone replacement therapy for low T, two of the most common delivery methods you will encounter are testosterone pellets and testosterone injections. Both treat clinically confirmed hypogonadism, but they differ significantly in how the hormone reaches your bloodstream, how often you need treatment, and what risks each method carries.
Testosterone injections
Testosterone injections deliver testosterone directly into muscle tissue or subcutaneous fat, with bioavailability approaching 95%. The most common forms are testosterone cypionate and testosterone enanthate, which are administered intramuscularly every one to two weeks in most protocols. Some providers now use subcutaneous injections, which are easier for self-administration and produce comparable pharmacokinetics. A 2022 systematic review in the Journal of Clinical Endocrinology and Metabolism found that subcutaneous testosterone therapy in doses similar to those given via the intramuscular route produces comparable mean serum testosterone levels, and may improve patient adherence due to easier self-administration. If needles concern you, that distinction matters.
Testosterone pellets
Testosterone pellets are small, rice-sized implants made of bioidentical testosterone that is chemically identical to the hormone your body naturally produces. A medical provider places them subcutaneously, typically in the upper buttock or hip area, through a small incision under local anesthetic. The pellets dissolve slowly, releasing testosterone at a controlled rate of about 1.5 mg per day over 3 to 6 months. Testopel is the only FDA-approved testosterone pellet; compounded pellets are also widely used in clinical practice. If you prefer fewer clinic visits and a more hands-off routine, you may find this delivery method appealing on the surface. But there are trade-offs worth understanding before you commit.
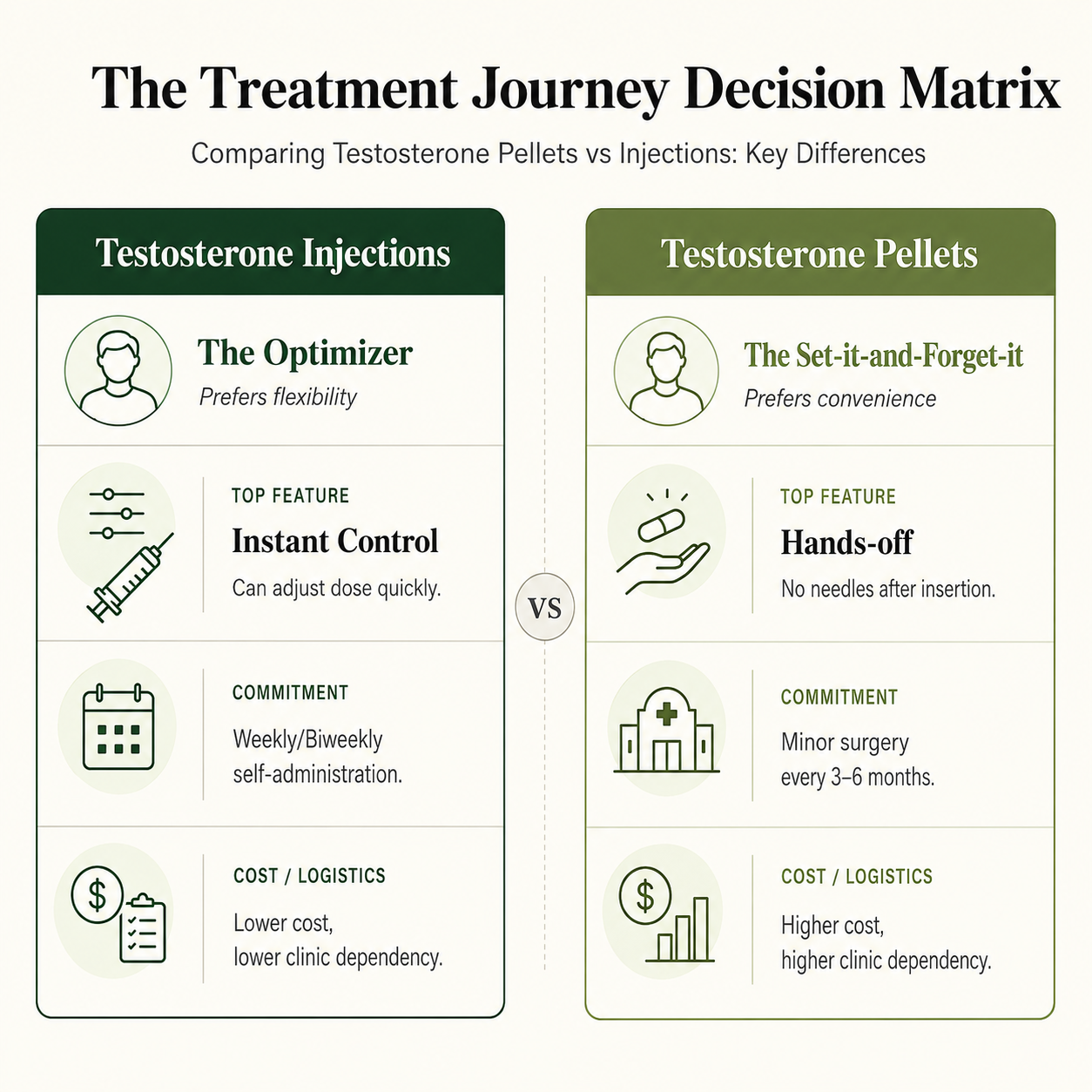
Comparing Testosterone Pellets vs Injections: Key Differences
| Feature | Testosterone Injections | Testosterone Pellets |
| Administration | Self-administered or clinic visit | Minor surgical procedure in clinic |
| Frequency | Weekly to biweekly | Every 3 to 6 months |
| Dose adjustability | Adjustable at any time | Fixed once implanted |
| Hormone level pattern | Peaks and troughs between doses | More steady level over time |
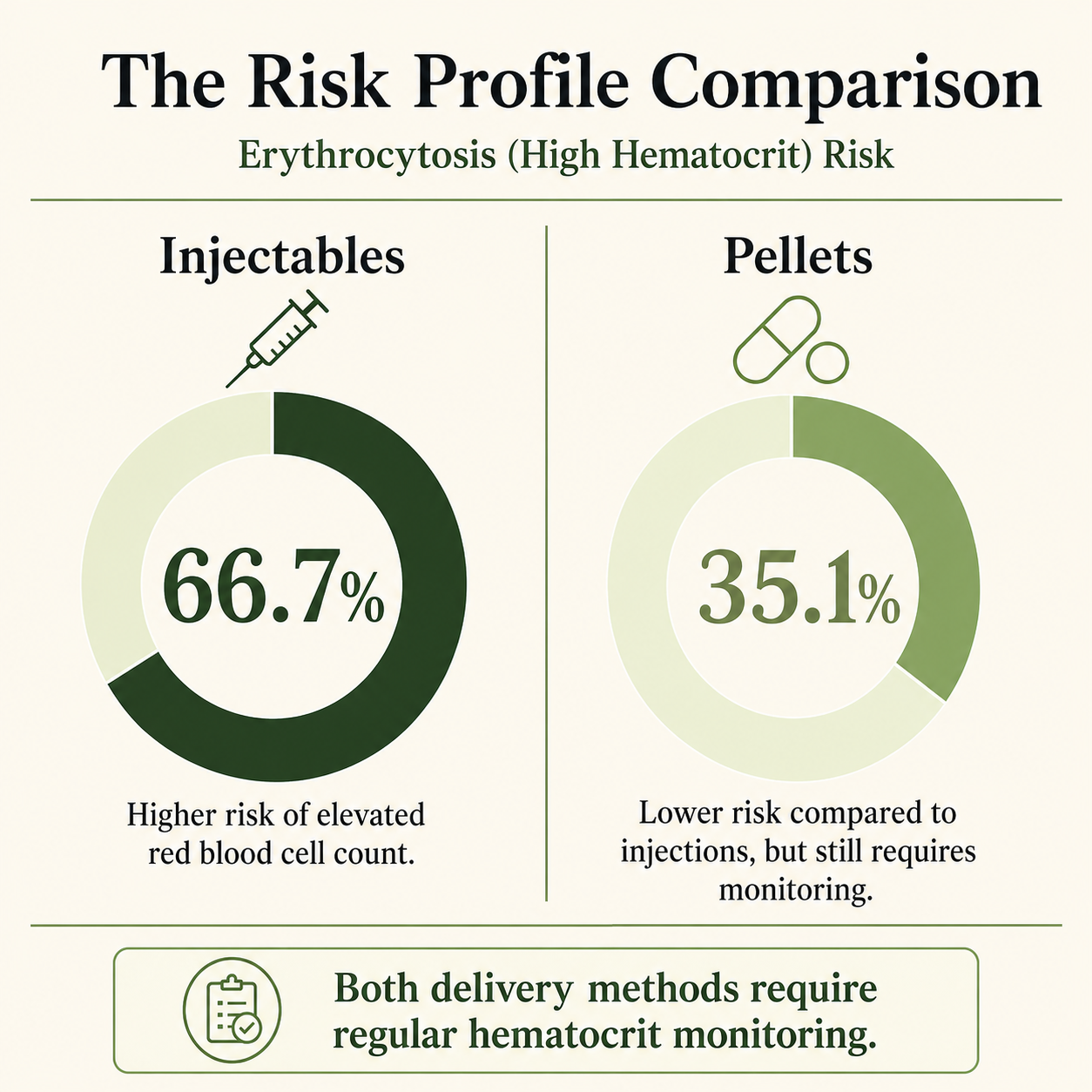
| Erythrocytosis risk | Higher (up to 66.7% in one study) | Lower (35.1% in same study) |
| Infection risk | Low (injection site reaction) | Small but present (1.2 to 5%) |
| Cost | Generally lower | Generally higher |
| Reversal | Immediate on stopping injections | Not reversible once inserted |
How Testosterone Injections Work
Testosterone injections deliver the hormone directly into muscle or subcutaneous tissue, from which it absorbs into your bloodstream. After an injection, your serum testosterone levels rise sharply, peaking within 24 to 72 hours depending on the ester used, and then gradually decline until the next dose. Levels also decline within days after stopping treatment. This pattern creates a cycle of elevated hormone levels followed by a drop.
If you are currently on weekly injections, you may recognize that trough period before your next dose. Research suggests many men report mood swings, fatigue, lower libido, and irritability in the days leading up to their next scheduled injection. These fluctuations are a well-recognized limitation of the injection process, and they are worth discussing with your provider if you experience them regularly, especially while finding the ideal dose.
Weekly injections using testosterone cypionate or enanthate at 100 to 200 mg are a standard approach in many clinics. Some protocols use more frequent, smaller doses, and some TRT injections are administered twice a week or even daily to reduce peak-to-trough variation. Subcutaneous injections, given into fat rather than muscle tissue, have gained traction as a more convenient and less uncomfortable option. If the injection process feels burdensome, that is a practical reason to discuss alternatives with your doctor.
How Testosterone Pellet Therapy Works
Testosterone pellet therapy works by delivering a slow, controlled release of testosterone directly from the implanted pellet under the skin into surrounding tissue and then into your bloodstream. Because the pellets dissolve gradually, your hormone levels tend to remain more stable over time compared to what you experience with weekly injections, though most men return for pellet re-implantation every 3 to 5 months rather than waiting a full 6 months.
Pellet insertion is an outpatient procedure. Your medical provider cleans the insertion site, injects a local anesthetic, makes a small incision, inserts several rice-sized implants, and closes the incision with adhesive strips or a suture. Most patients return to normal activity within a day or two. The number of pellets implanted, typically 8 to 14, is based on your body weight and baseline testosterone levels.
A prospective clinical trial published in the Journal of Sexual Medicine found that implantation of 900 mg of testosterone pellets (12 pellets) maintained serum testosterone at or above 300 ng/dL through 113 days, with most patients reporting satisfaction and improvement in depression scores, androgen deficiency symptoms, and sexual function. The study was small and open-label, which limits broader conclusions. You should know that before weighing it as strong evidence.
A survey of Sexual Medicine Society of North America members published in the Journal of Sexual Medicine found that the vast majority of clinicians implant at least 10 pellets per session, with high reported patient satisfaction rates and limited need for dose adjustment in subsequent cycles. If consistent dosing matters to your lifestyle, that finding may feel reassuring. But the inability to adjust mid-cycle is still a real limitation worth understanding. In practice, patients typically return for replacement every 3 to 5 months rather than reliably lasting a full 6 months.
Risks of Testosterone Injections
Testosterone injections carry real risks you should understand before starting treatment. Your provider should review these with you based on your personal health history.
Higher Risk of Elevated Hematocrit
Erythrocytosis (elevated hematocrit) is the most significant concern with injectable testosterone. Testosterone stimulates red blood cell production through several mechanisms, including suppression of hepcidin and stimulation of erythropoietin. When your hematocrit rises above 50 to 54%, blood viscosity increases, raising the theoretical risk of clotting events. A three-year retrospective study published in the journal Sexual Medicine found erythrocytosis in 66.7% of men using injectable testosterone, compared to 35.1% in the pellet group and 12.8% in the gel group. Injectable testosterone was also associated with earlier onset of erythrocytosis, at a mean of 10.5 months versus 16.4 months for pellets. If you have a history of cardiovascular concerns or elevated blood counts, this difference is clinically meaningful.
Increased Chance of Estradiol Elevation
Estradiol elevation is also more pronounced with injectable testosterone. The same three-year study found that increases in estradiol persisted throughout follow-up in the injectable group, while the pellet group showed estradiol increases that normalized after 6 months. Higher estradiol can contribute to fluid retention, breast tissue sensitivity, and mood changes in some patients. Aromatase inhibitors are used to manage these side effects, but they add complexity and cost to your treatment plan.
Injection Site Reactions
Injection site reactions are common and include pain, bruising, and localized inflammation. Intramuscular injections can be uncomfortable, particularly if you are self-administering for the first time. Subcutaneous administration appears to reduce discomfort but is not available through all clinics.
Hormone Peaks and Troughs Between Doses
Hormone fluctuations are an inherent limitation of injectable TRT. Your testosterone peaks shortly after injection and falls before the next dose. If you notice mood variability, irritability, anxiety, or reduced energy in the days before your next injection, that pattern is consistent with what the research describes as the trough effect.
Impact on Fertility
Fertility suppression occurs with all forms of exogenous testosterone. Injections suppress the hypothalamic-pituitary axis, which reduces your body's own testosterone production and sperm production. This effect is not limited to injections but applies equally to pellets and other forms. If preserving fertility is a priority for you, this is a critical conversation to have with your doctor before starting any form of TRT.
Risks of Testosterone Pellet Therapy
Pellet therapy introduces risks tied to the insertion procedure itself, as well as ongoing hormonal risks similar to other forms of TRT. You should not overlook the procedural side simply because the treatment feels more passive
Risk of Infection After Pellet Insertion
Infection at the insertion site is the most serious procedural risk. A comparative study in the Journal of Sexual Medicine reported infection rates of up to 5% with standard implantation technique, though modified techniques reduced this to approximately 1.2%. Because insertion is a minor surgery involving a small incision, there is also some risk of inflammation or scar tissue along with infection. Infections generally resolve without surgical intervention but require antibiotic treatment and close monitoring. You should ask your provider which technique they use and what their personal complication rates look like.
Pellet Extrusion and Unexpected Hormone Changes
Pellet extrusion occurs when your body pushes out one or more pellets through the incision before they dissolve. Rates range from under 1% to over 7% depending on technique, though with contemporary technique extrusion occurs in less than 3% of male procedures. Extrusion disrupts your dosing and may require a repeat procedure. If this happens to you, your hormone levels can drop unexpectedly mid-cycle.
Bleeding and Hematoma Formation
Hematoma formation at the insertion site can occur, particularly if you are on anticoagulants. Published reports also describe bleeding and bruising in approximately 8.8% of pellet procedures. Most cases in published data are resolved without additional surgical intervention, but it is still a risk worth disclosing to your provider before the procedure.
Limited Ability to Adjust Your Dose
Inability to adjust dose is a critical limitation that many patients do not fully appreciate beforehand. Once pellets are inserted, the dose cannot be changed or removed. If you develop an adverse reaction, elevated hematocrit, or unexpectedly high testosterone levels, there is no immediate way to reverse course. That is fundamentally different from injections, where your next dose can simply be withheld or reduced.
Risk of Elevated Hematocrit Over Time
Elevated hematocrit also occurs with pellets, though at lower rates than injections. The three-year study in Sexual Medicine found a 35.1% erythrocytosis rate with pellets at a hematocrit threshold of 50%. A separate retrospective study published in the Asian Journal of Andrology followed 228 men on testosterone pellet therapy and found that the estimated rate of erythrocytosis was 10.4% at 6 months, 17.3% at 12 months, and 30.2% at 24 months. If you are planning long-term pellet therapy, that cumulative trend is something you and your provider should monitor closely.
Higher Long-Term Treatment Costs
Cost is a practical consideration you should factor in early. The insertion procedure typically costs about $300 to $800, and pellet therapy can total roughly $2,600 per year, making this a more expensive option than weekly self-administered injections. Depending on your insurance coverage, out-of-pocket costs can vary significantly.
Hormone Level Stability: Pellets vs Injections
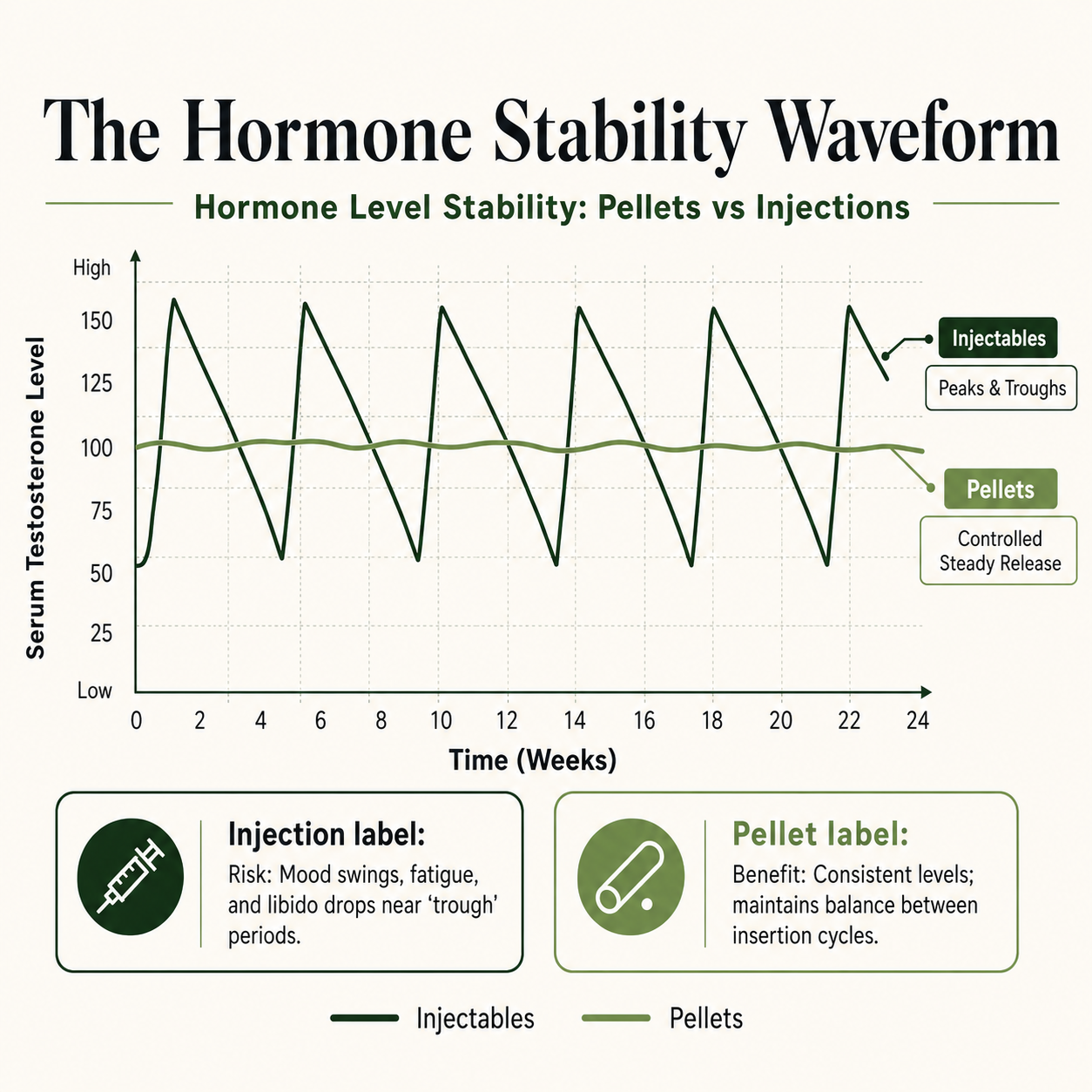
Stable hormone levels are one of the most frequently cited reasons patients and providers choose testosterone pellet therapy over weekly injections. If you have felt the highs and lows of injection cycles, that consistency may sound very appealing.
The three-year comparative study in Sexual Medicine confirmed that all testosterone formulations produced sustained increases in total and free testosterone throughout follow-up. However, mean testosterone levels were significantly higher in the injectable group than in the pellet or gel groups, which contributed to higher estradiol elevation and erythrocytosis rates in that group. You may find a steadier hormone level more comfortable day to day, but that stability also means you cannot quickly reduce your dose if something goes wrong between insertion cycles.
The practical implication is straightforward. If you experience significant symptom cycling on weekly injections, including mood swings, anxiety, or libido drops near your injection date, pellet therapy may reduce that variation. But if your levels run unexpectedly high after insertion, you will need to wait until the pellets dissolve before your levels normalize. That trade-off is worth discussing openly with your provider before making any decision.
What the Research Shows: Head-to-Head Comparisons
Direct, randomized comparisons between testosterone pellets and injections in large trials are limited. Most published data are retrospective, single-center studies with modest sample sizes. Here is what the available evidence actually tells you.
Injections Raise Testosterone Higher, But That Comes at a Cost
The three-year retrospective study published in Sexual Medicine from Baylor College of Medicine compared 74 men on pellets, 57 on injectable testosterone, and 47 on gels over 3 years. All formulations raised serum testosterone and provided sustained hormone replacement. Injectable testosterone produced higher total testosterone levels but also higher erythrocytosis rates and more persistent estradiol elevation. Pellets produced less erythrocytosis than injections but more than gels. No formulation significantly changed PSA levels in most patients. If your goal is maximizing testosterone numbers rather than clinical symptom relief, injections may achieve higher peaks. But you may be trading that for a higher hematocrit risk that requires regular monitoring.
Pellet Dosing Is Not a Set-It-and-Forget-It Solution
A 2023 randomized trial published in Sexual Medicine compared two types of testosterone pellets, compounded and branded, in 75 men with testosterone deficiency. Both achieved comparable testosterone levels. However, 82% of patients dropped below 300 ng/dL by the end of 6 months, suggesting that pellet dosing often requires re-titration sooner than the marketing implies. If you were told pellets last a full 6 months reliably, this finding is worth raising with your provider.
No Single Method Wins: The Evidence Supports an Individualized Approach
A 2021 review in Expert Opinion on Pharmacotherapy from the University of Miami concluded that each testosterone delivery method carries distinct advantages and disadvantages. The authors recommend that your treatment decision be individualized based on route of administration, efficacy, safety, and cost through a shared decision-making process with your provider, informed by clinical experience. That is not a hedge. It reflects the reality that your provider helps determine which option fits your clinical history, lifestyle, and risk tolerance so you can make an informed decision.
Pellet Therapy and Injections in Women
Both pellet therapy and injectable testosterone are also used in women, typically for low testosterone related to menopause, low libido, or hormonal deficiency after surgical menopause. If you are a woman considering either option, dosing is significantly lower than what is used in men. The same procedural risks apply to pellet insertion. This use is considered off-label by the FDA and has not been approved by the FDA for use in women. You should discuss those specifics directly with a provider experienced in female hormone therapy.
Who May Be Better Suited for Injections
Testosterone injections may be a better fit for you if:
- You prefer a lower-cost delivery method with more flexibility, especially if you want to fine-tune dosage and reach an ideal dose more easily
- You want the ability to adjust or stop treatment quickly if something changes, and that flexibility can support better health and overall well-being during dose optimization
- You do not experience significant symptoms tied to hormone fluctuations between doses
- You are comfortable with self-administration or regular clinic visits
- You have health conditions that make a minor surgical procedure inadvisable
Who May Be Better Suited for Pellet Therapy
Testosterone pellet therapy may be a better fit for you if:
- You experience significant symptom cycling on weekly injections and want a steadier level
- You prefer fewer clinic visits spread across 3 to 6 months
- You have stable, confirmed testosterone deficiency with predictable dosage needs, since adjustment is limited once pellets are placed under the skin
- You are comfortable with a minor surgery for insertion and understand the recovery
- You accept that dosing cannot be reversed or adjusted once pellets are inserted
How Testosterone Levels Are Properly Measured
Before you consider any delivery method, your testosterone deficiency needs to be confirmed through proper lab testing. Choosing a delivery method before confirming a diagnosis is skipping the most important step.
Proper evaluation means:
- A morning blood test with total testosterone drawn before 10 a.m.
- Repeat testing on at least two separate occasions for confirmation
- Free testosterone measurement if your total testosterone is borderline or your symptoms are strong despite a normal total T result
- Additional markers including LH, FSH, SHBG, and hematocrit as your provider sees fit
- Evaluation by a licensed medical provider who reviews your results in the context of your symptoms, not in isolation
If you are self-diagnosing based on fatigue or low libido alone, you may be missing other causes. Testosterone levels fluctuate with sleep quality, stress, illness, and time of day. The testing protocol matters, and getting it right before choosing a treatment path protects you from unnecessary therapy.
Frequently Asked Questions
Are testosterone pellets better than testosterone injections?
Neither is definitively better. Research shows both raise testosterone effectively, but pellets produce more stable hormone levels while injections carry higher erythrocytosis risk, and the best option is the one your provider helps determine from your labs, symptoms, and preferences so you can make an informed decision. The right choice depends on your individual health profile and clinical evaluation.
Testosterone pellets vs. injections: Which is better for seniors?
Pellets are typically preferable for seniors than injections since they have a lower erythrocytosis risk and older men have higher baseline hematocrit. BUT seniors shouldn't overlook injections' advantage: if you have a side effect or your levels are too high, your doctor can lower or stop the dose promptly, unlike with pellets. If you're taking blood thinners or controlling cardiovascular risk, flexibility may offset fewer clinic visits.
How long do testosterone pellets last compared to injections?
Pellets typically last 3 to 6 months, but most men require replacement every 3 to 5 months before levels decline and re-insertion is needed. Injections are given weekly or biweekly in most standard protocols.
Is pellet insertion a major surgical procedure?
No. Pellet insertion is a minor outpatient surgery performed under local anesthetic, not a major surgical procedure. It involves a small incision, placement of the pellets under the skin, and closure with adhesive strips. Most patients resume normal activity within 24 to 48 hours.
Do testosterone injections cause more mood swings than pellets?
Evidence suggests that the peaks and troughs of weekly injections can contribute to mood changes, irritability, and anxiety near the end of the dosing cycle. If you notice that pattern, it is worth discussing with your provider. Pellets may reduce that variation due to their controlled release delivery, though individual responses differ.
What is the infection risk with testosterone pellets?
Published data suggest infection rates of approximately 1.2 to 5% depending on insertion technique. Most infections resolve with antibiotics without requiring additional procedures. Ask your clinic about their specific complication rates before proceeding.
Can I switch from pellets to injections or vice versa?
Yes. A licensed provider can transition you between delivery methods. Timing the switch typically involves waiting until existing pellets have dissolved and your testosterone levels return toward baseline.
What is the cost difference between testosterone pellets and injections?
Injectable testosterone is generally less expensive. Compounded or generic injectable testosterone cypionate is among the most affordable forms of TRT. Pellets, including the insertion procedure, typically cost significantly more per cycle, though your insurance coverage will affect the final number.
Conclusion
Testosterone pellets and testosterone injections are both clinically used delivery methods for testosterone replacement therapy in men with confirmed low testosterone. Each has a distinct pharmacokinetic profile, risk profile, and set of practical considerations that affect your day-to-day experience on therapy.
Research consistently shows that injectable testosterone produces higher peak testosterone and estradiol levels and carries a greater risk of erythrocytosis compared to pellets. Pellets offer more stable hormone levels over months, but they require a minor surgical procedure, carry procedural risks including infection and extrusion, and cannot be reversed once inserted. Neither of those realities is a reason to avoid treatment. They are reasons to go into it with clear information.
No single method fits every patient. Your decision should be made together with a licensed medical provider, who can use your labs, symptoms, and clinical experience to help determine the better fit and support an informed decision. When low testosterone is properly diagnosed and monitored, the right treatment can support better health, well being, and overall well-being. If you are still weighing your options, use this article as a foundation for that conversation, not as a substitute for it.
Disclaimer
This content is for educational purposes only and does not replace medical advice. Testosterone therapy and hormone-related decisions should be guided by a licensed healthcare provider.
References
Kresch E, Lima TFN, Molina M, et al. Efficacy and safety outcomes of a compounded testosterone pellet versus a branded testosterone pellet in men with testosterone deficiency: a single-center, open-label, randomized trial. Sex Med. 2023;11(2):qfad007. doi:10.1093/sexmed/qfad007. PMID: 36936900. https://pubmed.ncbi.nlm.nih.gov/36936900/
Rotker KL, Alavian M, Nelson B, et al. Association of subcutaneous testosterone pellet therapy with developing secondary polycythemia. Asian J Androl. 2018;20(2):195-199. doi:10.4103/aja.aja_51_17. PMID: 29205178. https://pubmed.ncbi.nlm.nih.gov/29205178/
McMahon CG, Shusterman N, Cohen B. Pharmacokinetics, Clinical Efficacy, Safety Profile, and Patient-Reported Outcomes in Patients Receiving Subcutaneous Testosterone Pellets 900 mg for Treatment of Symptoms Associated With Androgen Deficiency. J Sex Med. 2017;14(7):883-890. doi:10.1016/j.jsxm.2017.04.734. PMID: 28673432. https://pubmed.ncbi.nlm.nih.gov/28673432/
Piecuch MJ, Patel BG, Hakim L, Wang R, Sadeghi-Nejad H. Testosterone Pellet Implantation Practices: A Sexual Medicine Society of North America (SMSNA) Member Questionnaire. J Sex Med. 2017;14(1):47-49. doi:10.1016/j.jsxm.2016.11.305. PMID: 27989489. https://pubmed.ncbi.nlm.nih.gov/27989489/
Figueiredo MG, Gagliano-Juca T, Basaria S. Testosterone Therapy With Subcutaneous Injections: A Safe, Practical, and Reasonable Option. J Clin Endocrinol Metab. 2022;107(3):614-626. doi:10.1210/clinem/dgab772. PMID: 34698352. https://pubmed.ncbi.nlm.nih.gov/34698352/
Kresch E, Patel M, Lima TFN, Ramasamy R. An update on the available and emerging pharmacotherapy for adults with testosterone deficiency available in the USA. Expert Opin Pharmacother. 2021;22(13):1761-1771. doi:10.1080/14656566.2021.1918101. PMID: 33866902. https://pubmed.ncbi.nlm.nih.gov/33866902/
Conners W, Flinn K, Morgentaler A. Outcomes with the "V" implantation technique vs. standard technique for testosterone pellet therapy. J Sex Med. 2011;8(12):3465-70. doi:10.1111/j.1743-6109.2011.02441.x. PMID: 21883944. https://pubmed.ncbi.nlm.nih.gov/21883944/
Pastuszak AW, Gomez LP, Scovell JM, et al. Comparison of the Effects of Testosterone Gels, Injections, and Pellets on Serum Hormones, Erythrocytosis, Lipids, and Prostate-Specific Antigen. Sex Med. 2015;3(3):165-173. doi:10.1002/sm2.76. PMID: 26468380. PMCID: PMC4599554. https://pmc.nlm.nih.gov/articles/PMC4599554/