The most effective way to lower hematocrit includes frequent blood donation, adjustment in TRT dosage, removing blood under medical supervision, or opting delivery methods. These methods may help you to avoid blood clots and improve oxygen delivery.
Men on TRT should monitor hematocrit at baseline before starting, at 3 months after initiation, at 6 months, and then annually. More frequent monitoring (every 4-6 weeks) is appropriate only after a therapeutic phlebotomy or a dose adjustment until levels stabilize.
Hematocrit isa measure of the percentage of blood made up of red blood cells. If any individual on TRT got hematocrit level of 45%, it means it is the total blood volume consisting of red blood cells. The rest is plasma and other components.
The hematocrit level is essential to maintain because red blood cells are responsible to carry oxygen throughout the body. Oxygen delivery is directly affected by change in hematocrit level. It is necessary for men on testosterone replacement therapy to keep the level lower to prevent blood thickness and blood clots in vessels.
How common is this? Elevated hematocrit affects an estimated 20-68% of men on TRT, making it the most common laboratory abnormality associated with testosterone therapy. Most men see hematocrit rise 3–8 percentage points above their baseline within the first 3–6 months of treatment.
In addition, it is important to know that a standard blood test often includes complete blood count CBC. The test is necessary to analyse a balance between plasma and red blood cell count. The human body regulates the balance. However certain factors like dehydration, testosterone therapy and certain medical conditions can disrupt the balance. This leads to thickens the blood and causes certain risk factors.
Disclaimer: All kinds of blood tests should only be done at medical prescription. All tests and ways to lower hematocrit should only be undertaken under the supervision of a qualified healthcare professional.
What are Normal vs Elevated Hematocrit Ranges?
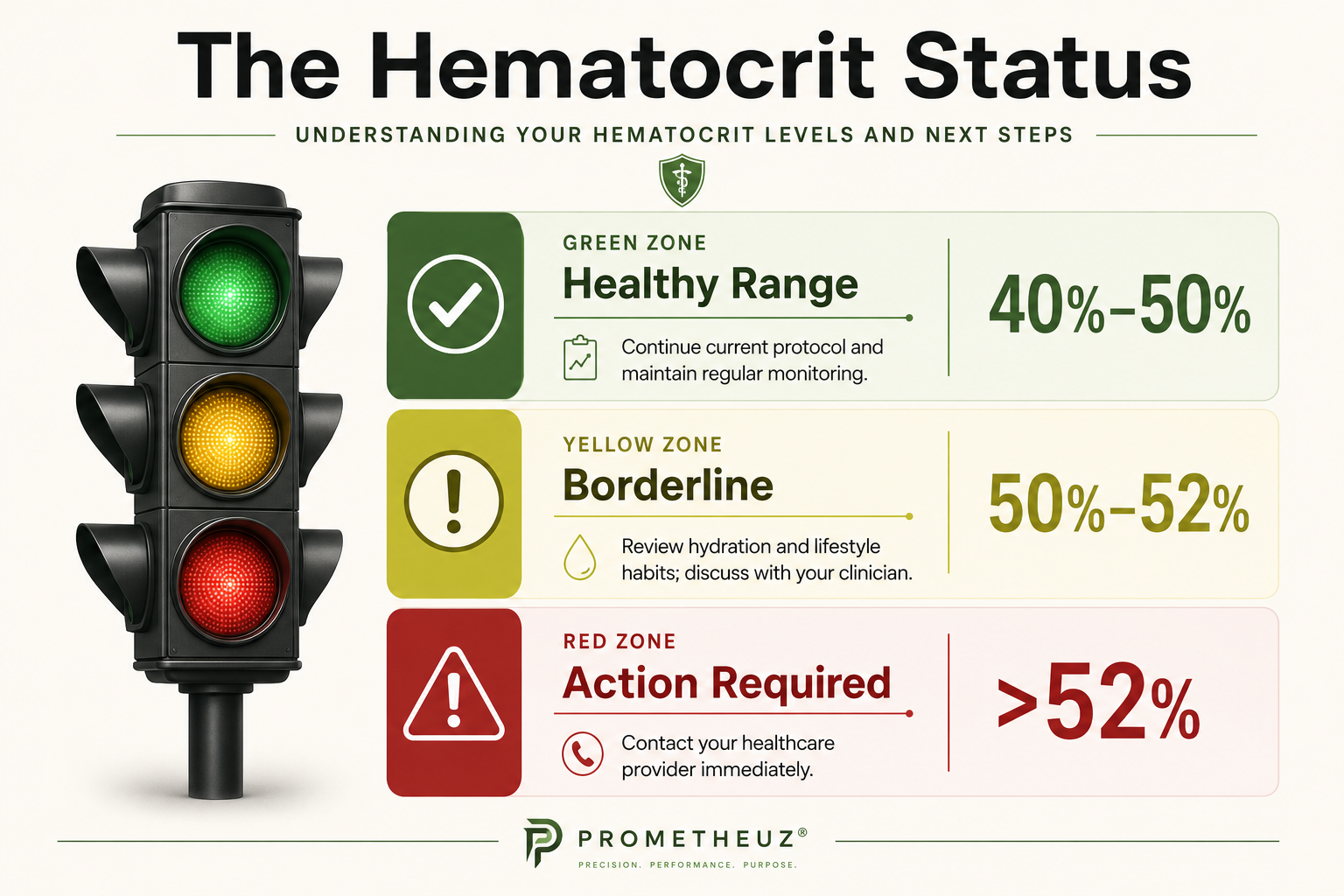
As per clinical suggestions, hematocrit’s normal level falls between 44% to 50% for men. The exact normal range can vary depending on the lab. If you are on TRT and got above 52%, you need to give attention. You may require medical consultation and steps to lower it down.
- Normal range: 41%–50%
- Monitoring range: 50%–52%
- Borderline elevated: 52%–54% (review protocol, increase monitoring frequency)
- Intervention threshold: Above 54% (Endocrine Society guideline: pause or reduce TRT until below 50%)
Single readings are less informative than trends. A hematocrit of 52% that has risen from 47% to 49% to 52% over three consecutive draws signals a trajectory requiring protocol review, even if 52% is within some labs' reference range. Your provider should be tracking the trend, not reacting to individual values in isolation.
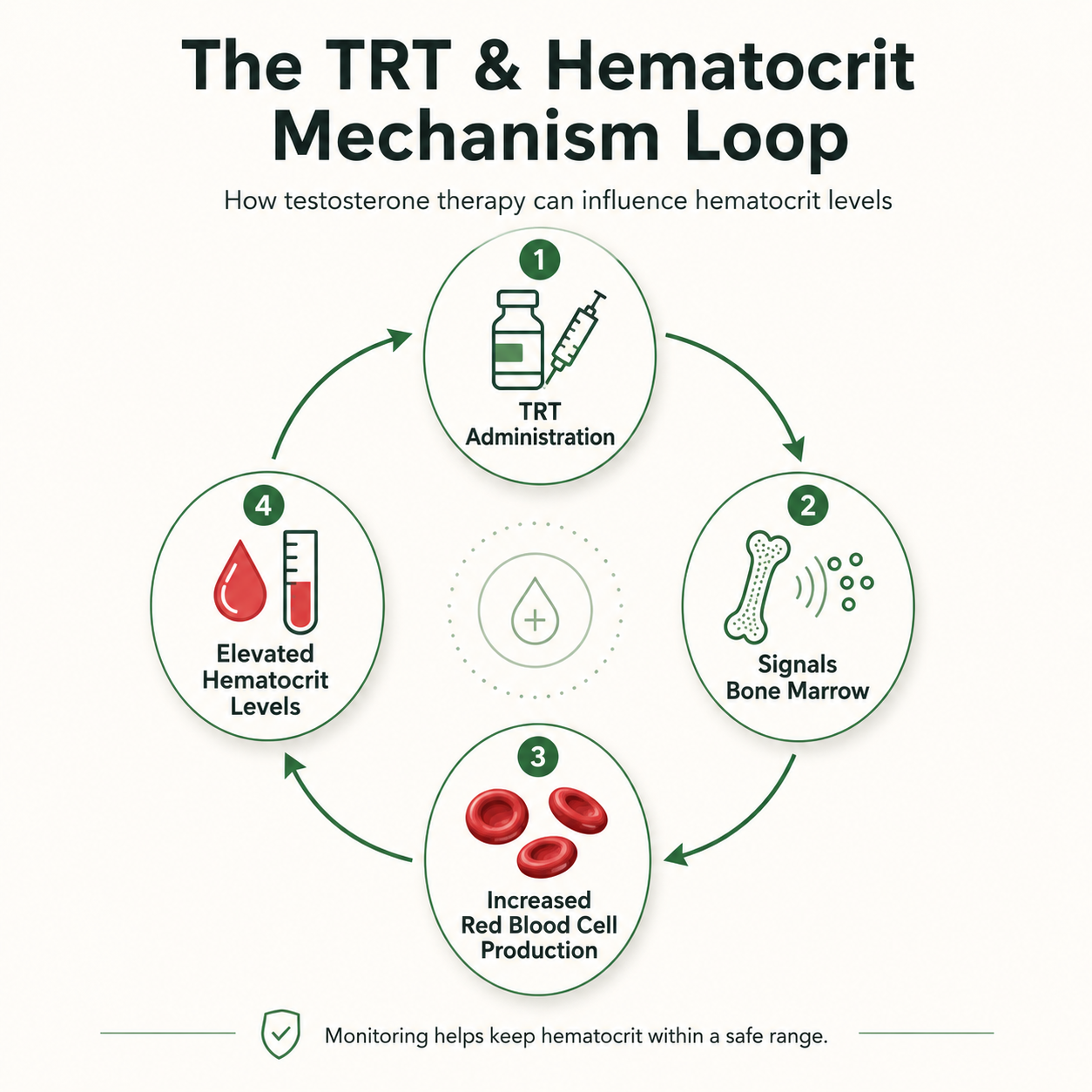
TRT plays a significant role in signaling the bone marrow to produce more red blood cells. This mechanism may boost energy and endurance. On other hand, individuals on testosterone replacement therapy TRT get elevated hematocrit by time. It is one of the side effects of men on TRT faces. In addition they need to monitor their hematocrit levels regularly.
Men on TRT may face:
- Increased red blood cells
- Raising hematocrit levels
- Blood clots
- Heart Attack
What Are Ways to Lower Hematocrit on TRT?
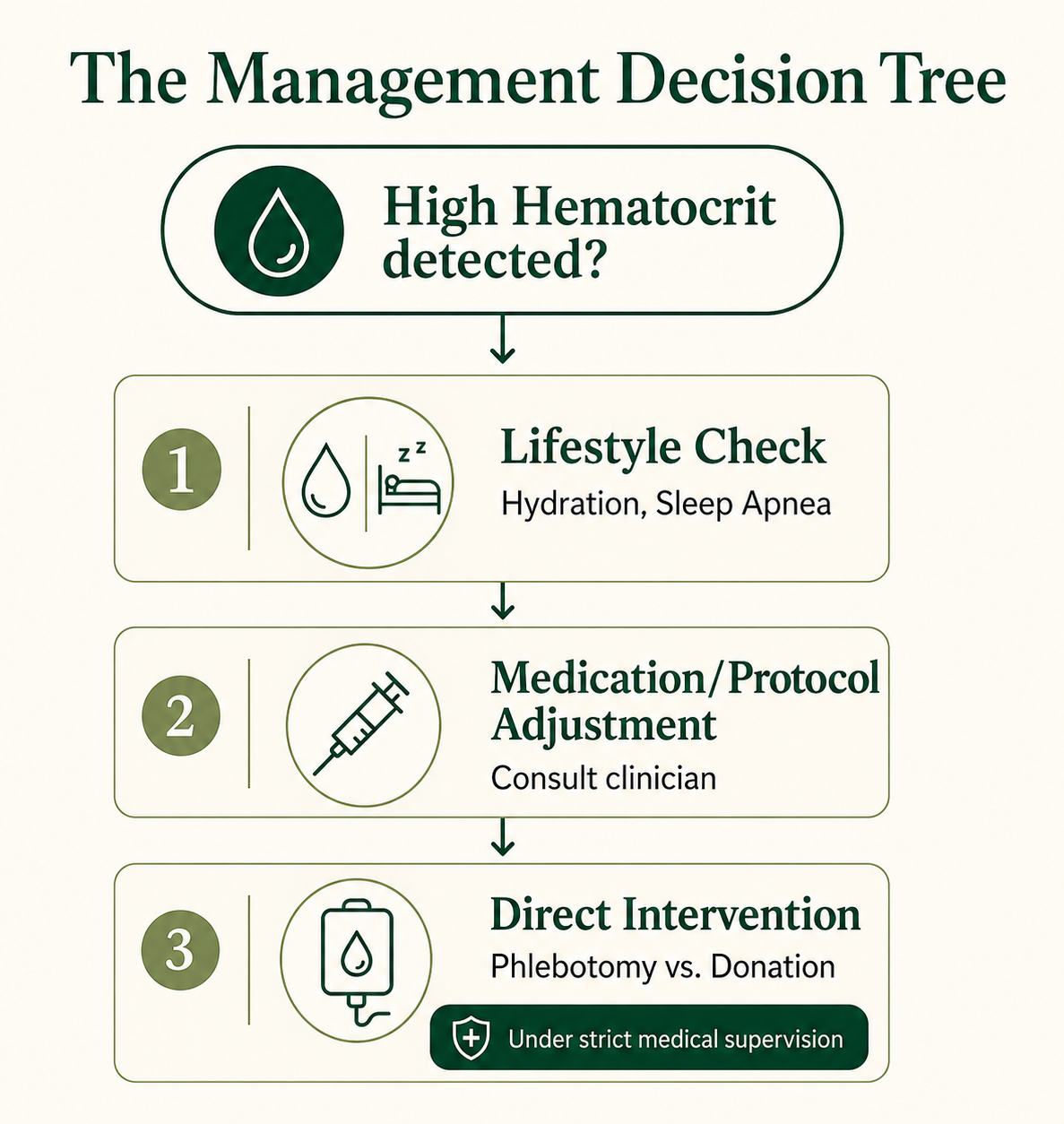
There are multiple ways men on TRT may opt to reduce hematocrit as per their medical specification. Here are some most common ways to follow under medical supervision:
Therapeutic Phlebotomy
Therapeutic phlebotomy is the fastest way to reduce Hematocrit. The procedure is more likely similar to blood donation. As per PMC, therapeutic phlebotomy is blood removal through venipuncture to treat high red blood cell count.
If an individual on TRT requires below 45% level then this clinical procedure is helpful under medical supervision. Patients are asked to stay hydrated, avoid heavy exercise and take rest after the procedure.
Risks
The procedure may cause dizziness, fatigue, bruising, and lightheadedness.
Blood Donation
Donating blood may work as an alternative to Therapeutic phlebotomy. Studies observed that a single blood donation may reduce approximately 3% of hematocrit levels. Standard whole blood donation removes approximately 470ml and drops hematocrit by roughly 3 percentage points within 1-2 weeks. The minimum interval between whole blood donations is 56 days (8 weeks) per American Red Cross guidelines, not 3-6 weeks. It is clinically suggested that in many cases only blood donation is not enough to maintain the 54% level.
Critical limitation
Blood donation removes red blood cells but does not address the underlying signals driving their production. If testosterone levels are still generating strong EPO stimulation, whether from dose, formulation, or co-existing sleep apnea, your body will regenerate those cells within 4-8 weeks. Men who find themselves donating every 8-12 weeks without stabilizing are treating the consequence, not the cause. Protocol adjustment to reduce peak testosterone exposure is the more durable solution in most cases.
In addition, to manage TRT most individuals need to choose an alternative procedure rather than blood donation.
Change TRT Delivery Methods
Sometimes medical professionals suggest individuals to try a change in delivery method. A study suggests a rise in testosterone may increase erythropoietin and bone marrow activity to raise red blood cells. Another study finding suggests that injectable ways of therapy may cause high levels of erythropoietin as compared to other methods.
A second mechanism operates through hepcidin suppression. Testosterone suppresses hepcidin, a hormone that normally limits iron absorption. Lower hepcidin means more iron enters circulation, which fuels red blood cell production independent of EPO stimulation. This is why blood donation alone often provides only temporary relief: it removes red blood cells but does not address the iron availability that drives their replacement.
Changing delivery methods is one of the most evidence-supported interventions for hematocrit management. High peak testosterone levels from biweekly intramuscular injections drive the greatest erythropoietin response. Switching to more frequent lower-dose injections or transdermal formulations reduces peak exposure and typically produces a meaningful reduction in hematocrit over 8-12 weeks.
Injection Frequency Adjustment (Without Reducing Total Dose)
Splitting a weekly injection into two or three smaller injections per week delivers the same total weekly testosterone dose while eliminating the high peak that drives erythropoiesis. For example, 100mg weekly can be split into 50mg twice-weekly or 33mg three-times-weekly. Many men see meaningful hematocrit reduction from frequency adjustment alone, without reducing total testosterone exposure or switching formulation.
As per above studies micro dosage, pellets and oral strategy may work better as compared to TRT injections.
| Delivery Method | Hormone Stability | Hematocrit Risk | Dosing Style | Key Insight |
| Injections | Low (peaks & crashes) | High | Weekly / biweekly | Spikes testosterone → increases red blood cell production |
| Creams / Gels | High (stable levels) | Low–Moderate | Daily | Steady absorption → lower erythropoiesis risk |
| Pellets | Moderate–High (slow release) | Moderate | Every 3–6 months | Stable but less flexible if hematocrit rises |