TRT vs No Treatment: Consequences of Untreated Low Testosterone
Untreated testosterone deficiency in men with clinical hypogonadism leads to significant health challenges, including reduced muscle mass, lower bone density, and increased metabolic risks. While Testosterone Replacement Therapy (TRT) can alleviate symptoms like low energy, mood changes, and sexual dysfunction, it carries medical risks such as suppressed sperm production and elevated hematocrit levels. The decision to pursue treatment requires clinical confirmation through morning blood tests, rather than self-diagnosis, as well as a thorough evaluation by a healthcare provider to weigh potential benefits against individual risk factors.
You feel it before you name it. Less energy in the afternoon. Fewer spontaneous erections. A bit weaker at the gym despite your best effort. These are common complaints in men over 40, and low testosterone levels often explain them.
The real question is: what happens if you do nothing, and what happens if you treat it? TRT vs no treatment is not a simple choice, and the answer is not the same for every man.
For men with confirmed testosterone deficiency a medical condition called male hypogonadism leaving low testosterone untreated is associated with a range of health consequences. For men experiencing age-related low testosterone without a confirmed clinical diagnosis, the picture is less clear. The data on treating functional or age-related declines is less robust, and the benefits are less predictable.
This article covers what the research shows about untreated low testosterone, the documented benefits and potential risks of testosterone replacement therapy, and how to think about both options with your healthcare provider.
What Is Low Testosterone and Who Actually Has It
Low testosterone means your testosterone levels have fallen below the normal range for healthy adult men. The generally accepted threshold is a total testosterone level below 300 ng/dL, confirmed on two separate morning blood test readings. Sometimes called "andropause" in popular media though this term is not used in clinical guidelines age-related testosterone decline is not an inevitable medical condition requiring treatment in every man. Age-related low testosterone also called late-onset hypogonadism (LOH) is a distinct clinical entity from primary or secondary hypogonadism. LOH typically presents with a slower, more gradual symptom onset and requires the same diagnostic confirmation before treatment is considered.
Male hypogonadism is the clinical term for a condition where your body cannot produce enough testosterone. It can stem from problems with the testes (primary hypogonadism) or the pituitary gland and hypothalamus (secondary hypogonadism). It is a recognized medical condition with established diagnostic criteria.
Age-related low testosterone is different. Your testosterone production declines naturally with age roughly 1 to 2 percent per year after age 30. Most of this decline is gradual and does not produce the same severity of symptoms seen in clinical hypogonadism. Normal aging does not automatically mean you need treatment.
Symptoms of low testosterone overlap with many other conditions. Fatigue, low libido, low sex drive, depressive feelings, loss of muscle mass, and erectile dysfunction can all have other causes, including sleep disorders, depression itself, cardiovascular disease, diabetes, and thyroid problems. This is why a blood test confirming low testosterone levels not symptoms alone is required before treatment is considered.
What Happens When You Leave Low Testosterone Untreated
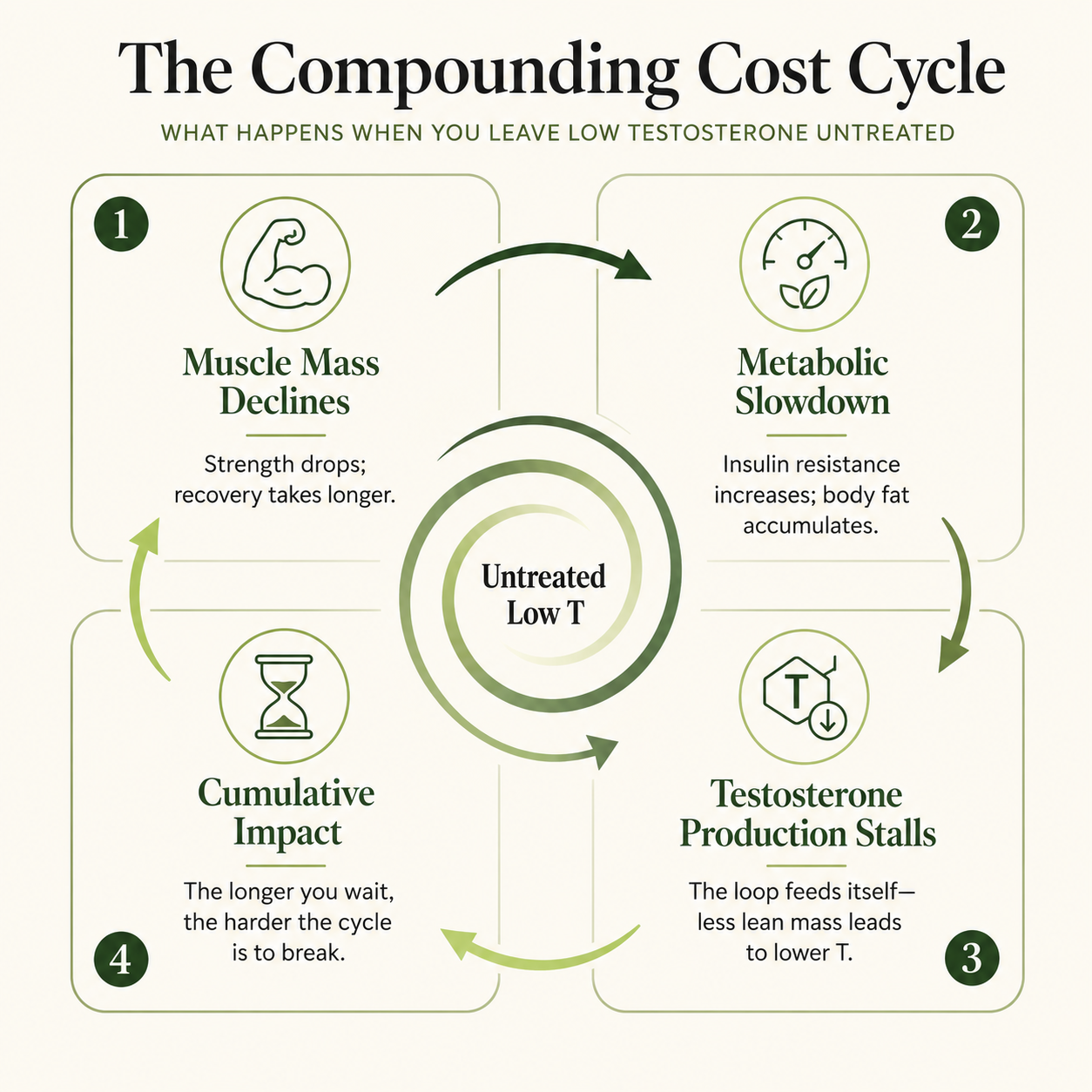
Untreated testosterone deficiency in men with clinical hypogonadism carries documented health consequences. You may not feel all of them at once. Many develop slowly, silently, and compound over years.
Your Body Composition and Bone Density
Testosterone plays a direct role in maintaining your muscle mass and bone mineral density. A review published in Advances in Experimental Medicine and Biology found that testosterone deficiency is associated with reduced lean body mass, increased fat mass, insulin resistance, metabolic syndrome, and reduced bone mineral density. Without adequate testosterone, you tend to accumulate more body fat and lose lean tissue over time even if your diet and training stay the same. It also influences secondary sex characteristics such as body hair, so deficiency can affect those features as well.
Reduced bone density increases your risk of fractures. You may not notice it for years. But it becomes clinically meaningful over time without treatment, and by the time you feel it, significant loss may have already occurred.
Your Sexual Function and Libido
Low testosterone levels are closely tied to your erectile function and sex drive. A clinical review in Clinics in Geriatric Medicine noted that testosterone deficiency is associated with reduced libido, erectile dysfunction, and decreased sexual satisfaction in men with hypogonadism. Erectile dysfunction is one of the most commonly reported symptoms you may experience, though it is not always caused by low testosterone alone, and psychological issues can also contribute to these symptoms and should be ruled out.
Untreated testosterone deficiency can also affect your sperm production. If you are planning to father children, this is a consequence worth discussing with your healthcare provider early, not after years of watchful waiting.
Your Mood and Energy
Depressive feelings, irritability, reduced motivation, emotional flatness, and fatigue are frequently reported by men with low testosterone. A 2024 study published in the Journal of Clinical Endocrinology and Metabolism found that more than half of hypogonadal men enrolled in the TRAVERSE trial had significant depressive symptoms at baseline before any treatment began. If you find yourself feeling persistently low without a clear reason, you may be experiencing the psychological weight of untreated testosterone deficiency.
Low energy and less energy during the day are among the most disruptive consequences. Men often describe a steady decline in drive and physical capacity that compounds over months or years without intervention.
Your Cardiovascular and Metabolic Health
Evidence suggests low testosterone levels may be independently associated with increased cardiovascular risk. A cohort study published in Basic and Clinical Andrology found that hypogonadal men who did not receive TRT had comparable rates of cardiovascular events to those who received treatment meaning the underlying condition itself carries risk, not only the treatment. The relationship between low testosterone and developing diabetes, insulin resistance, and metabolic syndrome is well-documented. If your testosterone levels are low and you also carry excess body fat, these two factors reinforce each other in a cycle that worsens over time without intervention.
Potential Risks of TRT: What You Need to Know Before You Start TRT
TRT is a medical treatment with documented risks. You deserve a clear, honest picture of each one before making any decision with your healthcare provider.
Sperm Production Suppression
When you introduce exogenous testosterone, your brain reads the elevated hormone levels and signals your testes to reduce their own production. This suppresses the hormonal signals necessary for sperm production, which means TRT can substantially reduce or eliminate your sperm count during treatment. If you intend to father children in the future, discuss fertility preservation options with your healthcare provider before therapy begins, not after, because if you later stop therapy, other symptoms may return while recovery of fertility can take time. Recovery of sperm production after stopping TRT typically takes 6 to 18 months and is not guaranteed in all cases duration of treatment and individual biology both influence recovery.
Elevated Hematocrit and Blood Clots Risk
Testosterone stimulates red blood cell production, which can push your hematocrit above the normal range. Thicker blood increases the potential risks of blood clots and downstream risks of stroke and pulmonary embolism. This is why a regular blood test is required during therapy and why most clinicians reduce the dose or pause treatment if your hematocrit climbs too high. Most clinical guidelines recommend reducing or pausing TRT if hematocrit exceeds 54%. Regular blood testing at 3 months and annually thereafter is the standard monitoring interval.
Worsening Sleep Apnea
TRT can worsen sleep apnea in men who already have it or unmask it in those previously undiagnosed. Testosterone may alter upper airway muscle tone and affect ventilatory drive during sleep. If you already have worsening sleep apnea or suspect you do, disclose this to your healthcare provider before starting untreated sleep apnea carries serious cardiovascular consequences of its own.
Prostate Growth and PSA Changes
A large randomized clinical trial published in JAMA Network Open involving over 5,200 hypogonadal men (the TRAVERSE trial) found no significant difference in prostate cancer incidence between TRT-treated men and placebo over a median follow-up of approximately 33 months reassuring news on prostate cancer risk. However, PSA levels did rise modestly in testosterone-treated men, which is why ongoing prostate monitoring remains necessary throughout treatment. Men with elevated PSA at baseline are not appropriate candidates for TRT.
Swollen or Tender Breasts and Skin Reactions
Testosterone converts to estrogen through a process called aromatization, which can cause swollen or tender breasts in some men, though a small number develop these side effects and they still matter clinically. The degree of conversion varies across individuals and can be tracked through your hormone levels. Testosterone medications delivered via gel or patch may also cause skin reactions at the application site, including redness and irritation.
Cardiovascular Disease Considerations
The cardiovascular picture has shown mixed results, and you should know that honestly. A review in Drug Safety noted that studies claiming increased heart attack risk often included undertreated or non-compliant patients, introducing confounding that distorted results. Current evidence does not confirm a significant increase in cardiovascular events with properly managed TRT in the short-to-medium term, although some earlier reports raised concerns about an increased risk of heart disease. That said, TRT is not appropriate if you have had a recent heart attack or have active unstable cardiovascular disease, and testosterone supplementation and overall testosterone use should be weighed against your individual cardiovascular history with a doctor, while heart health monitoring is appropriate for all men on therapy.
TRT Is Not the Same as Anabolic Steroids
Anabolic steroids are synthetic derivatives of testosterone used at supraphysiological doses without medical supervision to push muscle development far beyond what normal hormone levels support. TRT is the medical use of testosterone medications to restore your testosterone levels to the normal range. Framing TRT as equivalent to anabolic steroids misrepresents what supervised testosterone replacement therapy actually involves. Similarly, over-the-counter dietary supplements marketed to raise testosterone naturally have limited or no clinical evidence supporting meaningful effects on serum testosterone.
Testosterone Replacement Therapy vs. No Treatment: Weighing What It Costs You to Wait
You have already read about what untreated low testosterone does to your body. Now consider what it does to your life.
The TRAVERSE trial, the largest randomized controlled trial of TRT conducted to date, found that testosterone replacement therapy significantly improved sexual desire, erectile function, and overall sexual activity compared to placebo in hypogonadal men over 33 months of follow-up. Energy and mood improvements were also observed in men with confirmed deficiency. These findings are from a screened clinical population and do not extend to men without confirmed hypogonadism.
This is not about pushing you toward a decision. It is about helping you see the full picture because the consequences of low testosterone do not stay inside the gym or the bedroom. They follow you into the boardroom, the dinner table, and the mirror.
Go through each row honestly. If you recognize yourself in the left column, the right column is the direction things are heading without intervention. The final column is yours to mark.
Get clarity about your hormones.
Start with a private assessment, required lab work, and licensed clinician review.
| If you don't get treatment | What it costs you | You |
| Work: Brain fog becomes your baseline past midday | Missed deadlines. Slower thinking in meetings. Others start to notice before you do. | ☐ |
| Work: Your motivation drops. Starting tasks feels harder than finishing them. | You get passed over. Opportunities you would have chased start going to someone else. | ☐ |
| Work: Irritability creeps in. Your patience thins under pressure. | Your reputation shifts. You become the one people walk around, not toward. | ☐ |
| Relationships: Your low libido is lower than it used to be. Fewer spontaneous erections. | Distance builds. Your partner may assume it is about them. It usually is not. | ☐ |
| Relationships: You feel emotionally flat. Less engaged. Present in body, absent in energy. | Conversations get shorter. Connection fades quietly. Neither of you names it. | ☐ |
| Relationships: Depressive feelings make you withdraw. Social situations feel like effort. | Friendships thin out. You become harder to reach. People stop trying. | ☐ |
| Health: You are losing muscle mass despite training. Recovery takes longer. | Your body changes in ways you cannot reverse with effort alone. The gap between input and result widens. | ☐ |
| Health: You carry more body fat — especially around the midsection — without changing much. | Insulin resistance and metabolic risk increase. The longer you wait, the harder the cycle is to break. | ☐ |
| Health: Your energy is consistently low. You wake up tired. Afternoons are a write-off. | You compensate with caffeine and shortcuts. Nothing fixes the underlying problem. | ☐ |
Checking most of these boxes is not a diagnosis. It is a signal. Many of these symptoms have other causes, and marketing around low T can push men toward self-diagnosis before proper testing, so only a confirmed blood test interpreted by your healthcare provider can tell you whether low testosterone is driving them. But if this table describes your current life, that conversation is worth having sooner rather than later.
How Testosterone Levels Are Properly Measured
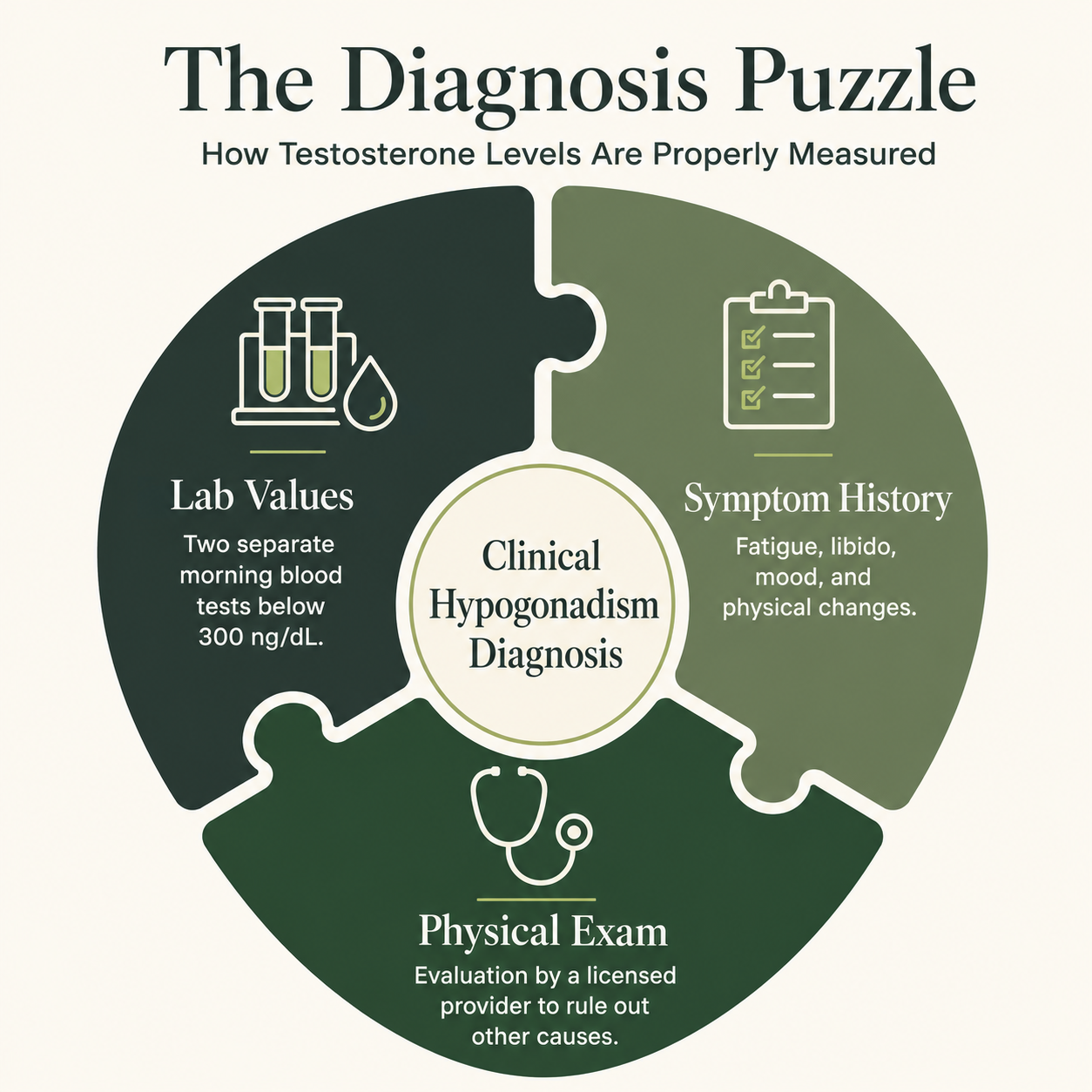
Diagnosis requires more than a single number, because symptoms and hormones must be assessed together rather than relying on one lab value. A proper evaluation involves the following.
Morning Blood Testing for Accurate Results
Total testosterone is the standard first measurement. A morning blood test is required. Your testosterone levels peak in the early morning hours and decline through the day. Testing in the afternoon can produce artificially low readings.
Confirming Low Testosterone With Repeat Testing
Repeat testing is required to confirm low testosterone. A single low result is not sufficient for diagnosis. Two separate blood test readings below 300 ng/dL, drawn on different days under consistent conditions, are needed to confirm deficiency rather than treat men who are already within normal levels.
When Free Testosterone Testing Is Needed
Free testosterone may be measured if your total testosterone is borderline or if SHBG (sex hormone-binding globulin) is suspected to be elevated. Free testosterone represents the biologically active fraction.
Using LH and FSH to Identify the Cause
LH and FSH help distinguish primary from secondary hypogonadism and guide treatment decisions.
All of these factors must be evaluated by a licensed healthcare provider. No blood test alone diagnoses hypogonadism; your results must be interpreted alongside a full symptom history and physical examination, and a doctor may also use guideline-based recommendations, including those from the American College, when deciding whether treatment is appropriate.
Lifestyle and the Underlying Cause of Low Testosterone
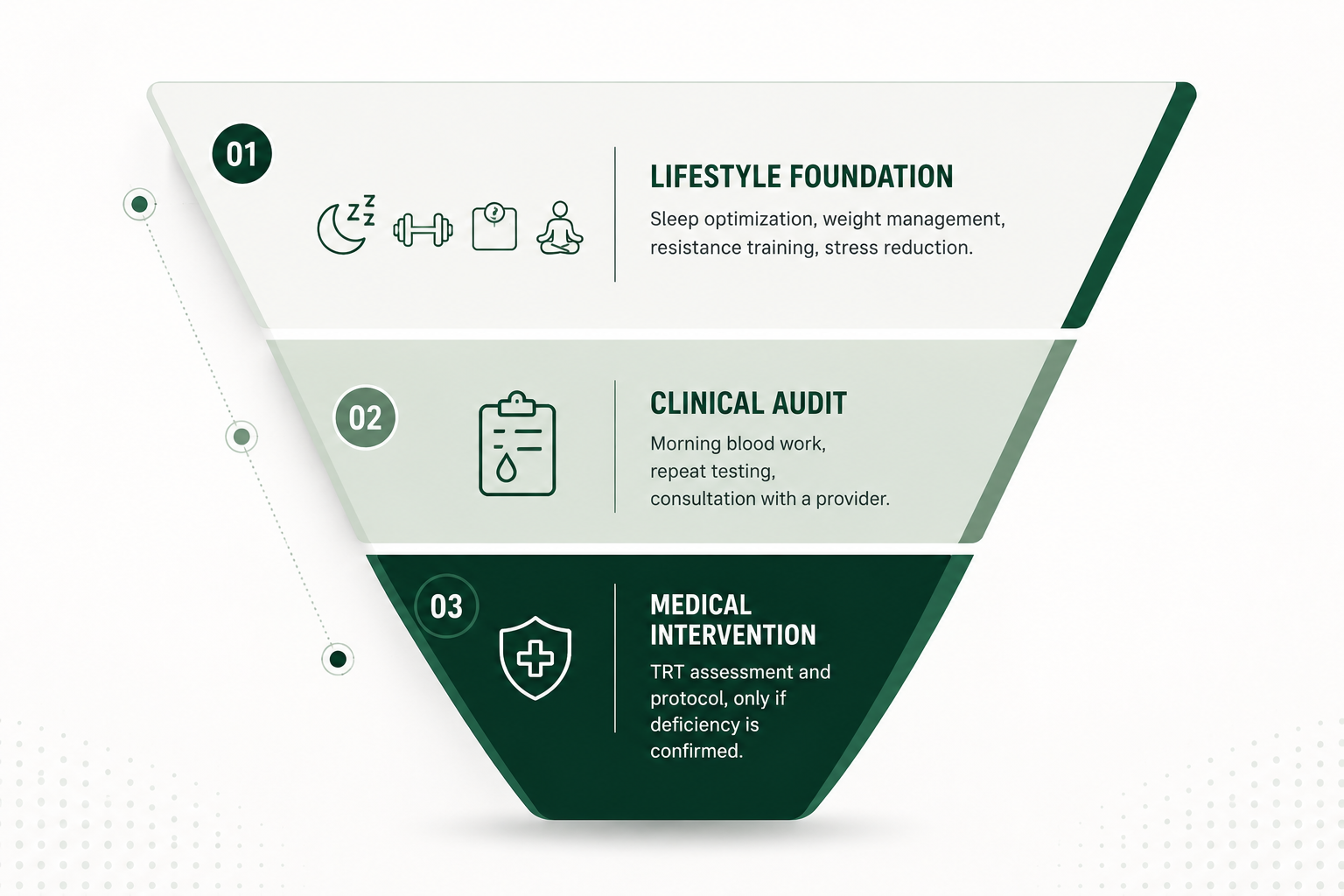
Before considering testosterone replacement, addressing the underlying cause matters. You may be able to shift your hormone levels meaningfully without medication but only if a modifiable cause is actually driving your low testosterone.
Weight Loss Can Improve Testosterone Levels
Obesity is one of the most common drivers of low testosterone in adult men. Your adipose tissue converts testosterone to estrogen. Meaningful weight loss can raise your testosterone levels without medication. Research suggests a 10% reduction in body weight can produce clinically significant increases in testosterone levels.
Sleep Is Essential for Testosterone Production
Sleep plays a central role. Most of your testosterone production occurs during deep sleep. If you are sleeping fewer than six hours per night, you are likely suppressing your morning testosterone readings. Poor sleep quality, including undiagnosed sleep apnea, directly limits testosterone production.
Strength Training Supports Hormonal Health
Resistance training supports testosterone production. Regular strength-focused exercise elevates anabolic hormone levels and preserves muscle mass. The effect compounds over time when you stay consistent.
Managing Stress to Protect Testosterone Levels
Stress and cortisol suppress testosterone through the hypothalamic-pituitary axis. If you are chronically stressed, your cortisol stays elevated and that directly inhibits testosterone production. Stress management is not optional if you are trying to support your hormonal health.
Correcting Vitamin D Deficiency
Vitamin D deficiency is associated with lower testosterone levels. If you are deficient and you correct it, you may see modest improvement in your hormone levels.
When Lifestyle Changes Are Not Enough
If your symptoms persist after meaningful lifestyle changes over a sustained period, clinical evaluation is the appropriate next step. If a blood test confirms low testosterone levels consistent with male hypogonadism, a licensed provider may discuss options including TRT.
Frequently Asked Questions
What is the difference between TRT and taking anabolic steroids?
TRT restores your testosterone levels to the normal range because of a confirmed medical condition. Anabolic steroids are used at supraphysiological doses without medical supervision to push testosterone far above normal. They are not the same thing.
Will TRT permanently shut down my natural testosterone production?
TRT suppresses your body's own testosterone production while you are on it. It may be delivered by methods such as injections, but suppression occurs regardless of delivery method. Whether this suppression becomes permanent depends on duration of use, dosing, and your individual biology. Most men can recover natural testosterone production after stopping, but recovery takes time and is not guaranteed in all cases. Discuss this with your healthcare provider before you start, which is one reason stopping treatment should be planned with a doctor rather than done casually.
Can I raise testosterone naturally enough to avoid TRT?
If you have age-related low testosterone and lifestyle-modifiable factors, meaningful improvements are possible through weight management, sleep, exercise, and stress reduction. If you have clinical hypogonadism from a structural or genetic cause, lifestyle changes alone are unlikely to normalize your testosterone levels.
Is testosterone therapy safe for my heart health?
Current short-to-medium-term trial data does not support a significant increase in cardiovascular events with TRT in carefully managed patients. However, TRT is not appropriate if you have had a recent heart attack or have unstable cardiovascular disease. Heart health monitoring remains appropriate for all men on therapy.
How long before I notice effects from TRT?
Effects vary by symptom. You may notice sexual function and mood changes within weeks. Body composition changes take months. Bone density improvements require a year or more. There is no universal timeline.
Does TRT cause prostate cancer?
A major randomized clinical trial found no significant difference in prostate cancer incidence between TRT-treated men and placebo-treated men in a screened population. TRT does raise PSA modestly, which requires monitoring. If you have known or suspected prostate cancer, you are not a candidate for TRT.
What happens if I stop TRT?
When men stop therapy, testosterone typically returns toward pre-treatment levels over weeks to months. Symptoms that improved on therapy often return, and any benefits usually fade as levels fall back, especially if the underlying deficiency remains untreated. Do not abruptly manage discontinuation with your healthcare provider.
Conclusion
The decision between TRT vs. no treatment is not a binary choice between optimal health and stagnation. It is a medical decision that depends on whether you have confirmed testosterone deficiency, the severity of your symptoms, your underlying health conditions, and your goals.
If you leave low testosterone untreated and you have true male hypogonadism, the consequences accumulate. Your muscle mass declines. Your energy flattens. Your mood shifts. Your relationship and your performance at work can take quiet hits that you may not connect back to your hormone levels.
Testosterone treatment offers documented benefits for men who meet diagnostic criteria. It also carries real risks that must be weighed honestly and managed with proper clinical oversight. The data does not support using testosterone replacement casually or without confirmed need.
If you are experiencing symptoms that match what has been described here, the right starting point is a morning blood test, a repeat confirmation, and an honest conversation with a licensed healthcare provider about what your numbers actually mean.
Disclaimer
This content is for educational purposes only and does not replace medical advice. Testosterone therapy and hormone-related health decisions should be guided by a licensed healthcare provider.
References
Bassil N, Alkaade S, Morley JE. The benefits and risks of testosterone replacement therapy: a review. Ther Clin Risk Manag. 2009;5:427-448. doi:10.2147/tcrm.s3025. PMCID: PMC2701485. https://pmc.ncbi.nlm.nih.gov/articles/PMC2701485/
Bassil N, Morley JE. Late-life onset hypogonadism: a review. Clin Geriatr Med. 2010;26(2):197-222. doi:10.1016/j.cger.2010.02.003. PMID: 20497841. https://pubmed.ncbi.nlm.nih.gov/20497841/
Bhasin S, Seidman S, Travison TG, et al. Depressive Syndromes in Men With Hypogonadism in the TRAVERSE Trial: Response to Testosterone-Replacement Therapy. J Clin Endocrinol Metab. 2024;109(7):1814-1826. doi:10.1210/clinem/dgae026. PMID: 38205962. https://pubmed.ncbi.nlm.nih.gov/38205962/
Bhasin S, Travison TG, Pencina KM, et al. Prostate Safety Events During Testosterone Replacement Therapy in Men With Hypogonadism: A Randomized Clinical Trial. JAMA Netw Open. 2023;6(12):e2348692. doi:10.1001/jamanetworkopen.2023.48692. PMID: 38150256. https://pubmed.ncbi.nlm.nih.gov/38150256/
Hackett GI. Testosterone Replacement Therapy and Mortality in Older Men. Drug Saf. 2016;39(2):117-130. doi:10.1007/s40264-015-0348-y. PMID: 26482385. https://pubmed.ncbi.nlm.nih.gov/26482385/
Pantalone KM, George J, Ji X, et al. Testosterone replacement therapy and the risk of adverse cardiovascular outcomes and mortality. Basic Clin Androl. 2019;29:5. doi:10.1186/s12610-019-0085-7. PMID: 30976419. https://pubmed.ncbi.nlm.nih.gov/30976419/
Traish AM. Negative Impact of Testosterone Deficiency and 5-alpha-Reductase Inhibitors Therapy on Metabolic and Sexual Function in Men. Adv Exp Med Biol. 2017;1043:473-526. doi:10.1007/978-3-319-70178-3_22. PMID: 29224108. https://pubmed.ncbi.nlm.nih.gov/29224108/