TRT is available in five main formulations: injectable testosterone (cypionate, enanthate, undecanoate, propionate), transdermal gels and creams, oral testosterone undecanoate, nasal gel, and subdermal pellets. Each differs in how often it is administered, how stable blood levels remain, and whether needles are required. Injectable testosterone cypionate is the most commonly prescribed form in the United States.
Have you ever wondered why some men get testosterone injections every two weeks while others use a daily gel? Or whether one option actually works better than the other?
Testosterone affects more than just muscle mass and low libido. It shapes energy, mood, mental clarity, and overall well-being. When levels fall below normal, the symptoms can affect every part of daily life. The right form of testosterone therapy can make treatment more effective and easier to stick with.
This guide covers every major form of testosterone replacement therapy. It explains how each one works, what the research says, and how to have a more informed conversation with your healthcare provider.
What Are the Different Types of Testosterone?
Testosterone replacement therapy comes in five main delivery categories. These are injectable, transdermal, oral, nasal, and subdermal. Each category includes specific formulations with different release profiles and administration methods.
A review published in Andrology found that over decades of clinical use, numerous formulations have been developed to improve pharmacokinetics and patient compliance across all delivery routes. The goal in each case is the same: restore serum testosterone to within the normal physiologic range and relieve the symptoms of testosterone deficiency.
Injectable Testosterone: The Most Common Forms
Injectable testosterone is the most widely used form of testosterone replacement therapy test. These testosterone injectables include several injectable forms that deliver testosterone directly into muscle or subcutaneous tissue. From there, it is slowly released into the bloodstream.
A review in Translational Andrology and Urology found that injectable testosterone esters are modified forms of testosterone designed to extend the hormone's active time in the body, an ester change that makes this medication practical for ongoing treatment. Without modification, testosterone breaks down too quickly to be therapeutically useful.
Testosterone Cypionate
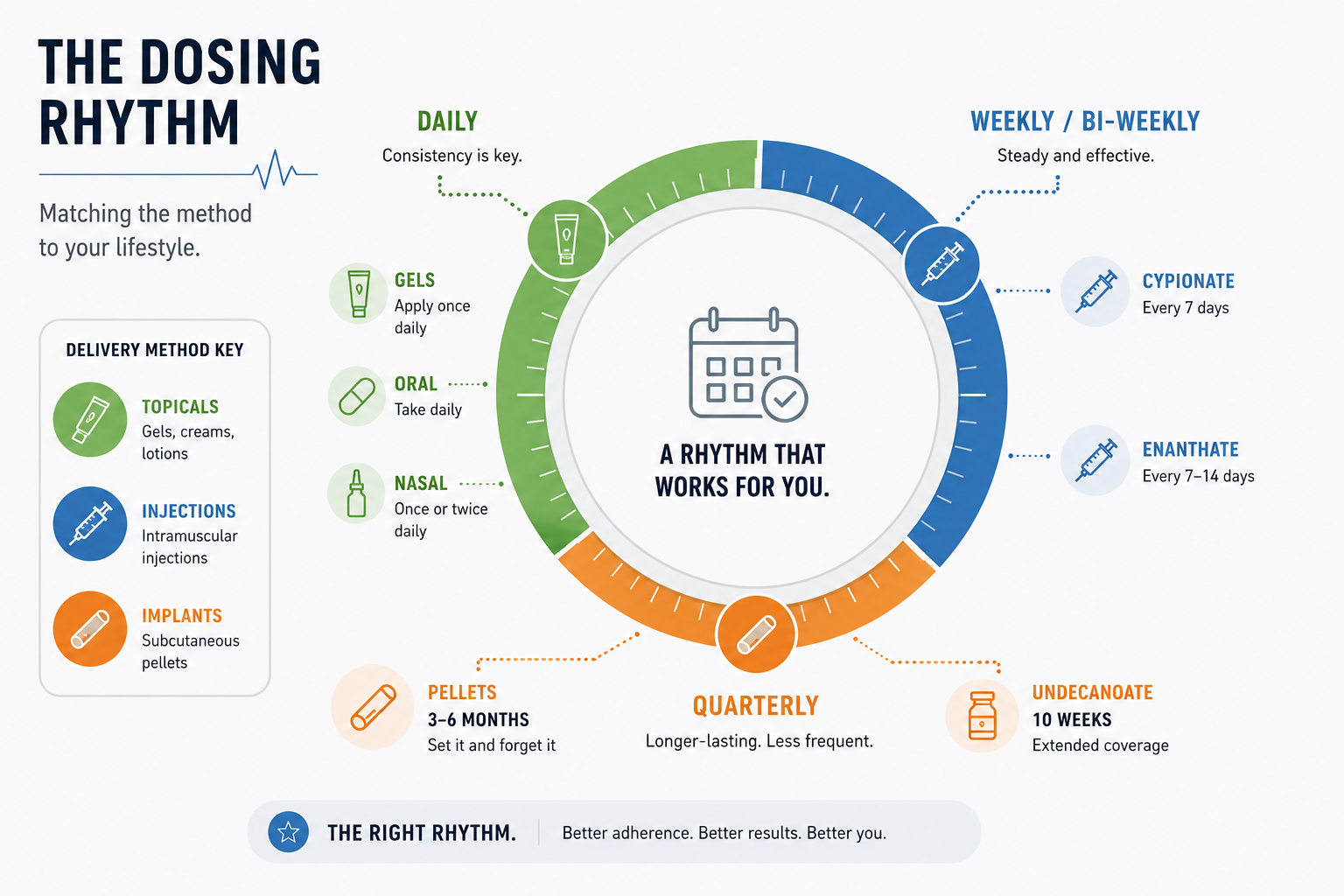
Testosterone cypionate is the most widely prescribed injectable testosterone in the United States. It has a half-life of approximately eight days. This gives it a longer window between doses compared to many other options.
It is typically injected into the gluteal muscle every one to two weeks. Many providers use smaller, more frequent injections to keep blood levels more stable throughout the treatment period. It can also be given as a subcutaneous injection into the abdomen or upper arms, which some patients find easier to manage at home.
Testosterone cypionate can be self-administered after proper training from a healthcare provider. Its availability, flexibility, and lower cost make it one of the most practical options for long-term testosterone replacement therapy.
Testosterone Enanthate
Testosterone enanthate works in a similar way to testosterone cypionate. Its half-life is slightly shorter, at around five to seven days. This means some patients need more frequent injections to maintain consistent blood levels.
It is available in both intramuscular and subcutaneous forms, with the injection site varying by route. One subcutaneous version is injected weekly into the abdomen and tends to produce more stable hormone levels compared to larger biweekly doses.
Testosterone enanthate also has a broader range of approved clinical uses. In addition to treating low testosterone in adult men, it is used for adolescents with delayed puberty and women with certain types of metastatic breast cancer.
Testosterone Undecanoate (Injectable)
Injectable testosterone undecanoate has the longest duration of any injectable testosterone formulation. After an initial loading phase, it is administered once every ten weeks. This makes it the most convenient option for men who want fewer injections.
However, this formulation must be given by a healthcare provider in a clinical setting. It carries a rare but serious risk called pulmonary oil microembolism, where small oil droplets from the injection can enter the lungs. Patients are monitored for 30 minutes after each dose as a precaution.
Testosterone Propionate
Testosterone propionate is a short-acting injectable form of testosterone. Its half-life is roughly two to three days, which means it requires injections every two to three days to maintain stable testosterone levels.
Because of this frequency, testosterone propionate is rarely the first choice today. Longer-acting formulations have largely replaced it in routine clinical practice. It is still used in some countries and in specific clinical situations where short-acting control is needed.
Injectable Testosterone Comparison Table
| Type | Half-Life | Injection Frequency | Self- Injectable | Key Notes |
| Testosterone Cypionate | ~8 days | Every 1-2 weeks | Yes | Most widely prescribed in the US. Flexible dosing. Lower cost. Strong safety record. |
| Testosterone Enanthate | ~5-7 days | Every 1-2 weeks | Yes | Similar to cypionate. Broader approved uses. Weekly subcutaneous option available. |
| Testosterone Undecanoate | ~34 days | Every 10 weeks | No | Fewest injections. Must be given in the clinic. POME risk requires monitoring. |
| Testosterone Propionate | ~2-3 days | Every 2-3 days | Yes | Rapid onset. Requires most frequent injections. Less common in modern TRT practice. |
Testosterone Cypionate vs Testosterone Enanthate: Key Differences
Both are esterified testosterone injectables that work the same way in the body. The ester chain is the only structural difference, and it produces a modest variation in half-life. For most men, the choice comes down to availability and dosing preference rather than clinical superiority.
One data update to flag: Testosterone cypionate has been on the ASHP drug shortage list since early 2023, with supply remaining intermittent as of 2026. If cypionate is unavailable at your pharmacy, enanthate is a direct substitute at the equivalent dose.
| Feature | Testosterone Cypionate | Testosterone Enanthate |
| Ester chain | 8-carbon | 7-carbon |
| Half-life | ~8 days | ~5-7 days |
| Active testosterone per 100mg | ~69 mg | ~70 mg |
| Typical carrier oil | Cottonseed or grapeseed oil | Sesame oil (thicker; may cause more injection site discomfort) |
| Typical injection schedule | Every 1-2 weeks or twice weekly | Every 1-2 weeks or twice weekly |
| Subcutaneous option | Yes | Yes |
| Self-injectable | Yes | Yes |
| FDA-approved indications | Hypogonadism in adult males | Hypogonadism in adult males; delayed puberty in adolescents; certain metastatic breast cancer cases in women |
| Generic availability | Yes - most commonly stocked in US pharmacies | Yes - less common in US; standard in Europe |
| Typical out-of-pocket cost (generic) | ~$30-$112/month | ~$84-$153/month |
| Supply status (2026) | Intermittent shortage reported | Generally available |
Bottom line: Either formulation produces equivalent testosterone levels under proper clinical management. Cypionate's longer half-life suits less frequent dosing; enanthate's slightly shorter half-life works well for twice-weekly protocols. If your pharmacy cannot fill cypionate due to the ongoing shortage, enanthate at the same weekly dose is a direct substitute. Confirm the switch with your provider and recheck labs at six to eight weeks.
Testosterone Gels and Transdermal Forms
Testosterone gels are applied directly to the skin, usually on the upper arms, shoulders, or inner thighs. They are typically applied once daily, and the skin absorbs the hormone gradually throughout the day, which provides a relatively steady daily release. Transdermal patches are another skin-based option and provide a consistent daily release of testosterone.
FDA-approved testosterone gels available in the United States include AndroGel (1% and 1.62%), Testim, and Vogelxo. Transdermal patches include Androderm.
Daily application is required. This suits men who want to avoid injections entirely, but it does require a consistent daily routine, and users need to let the product dry before dressing.
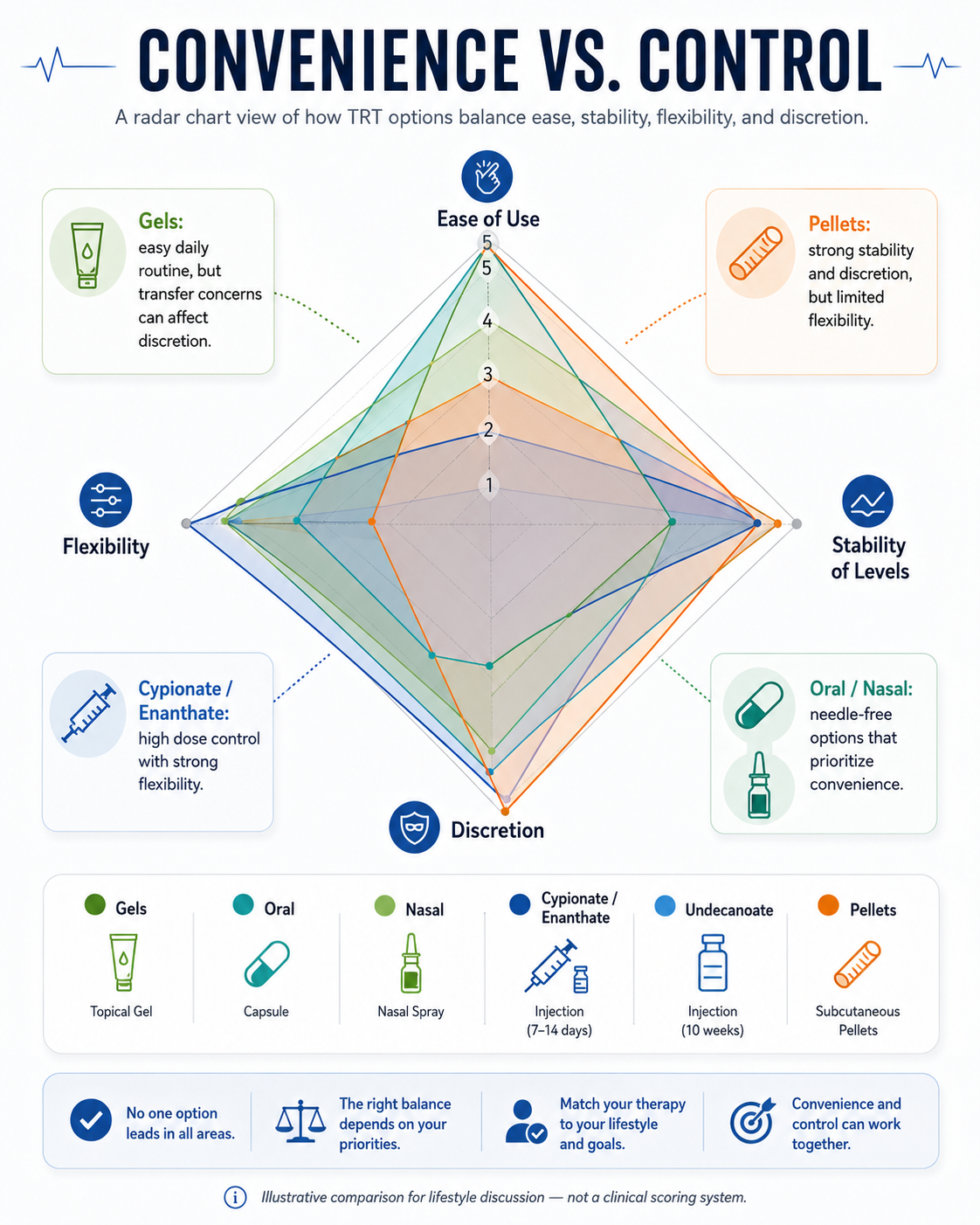
One important consideration is skin contact transfer. If a gel user makes physical contact with a child or partner before the application site has dried and been covered, testosterone can transfer through skin contact. Washing hands thoroughly and covering the site after application reduces this risk. Topical testosterone may also offer benefits in men who prefer a low risk of side effects compared with injections, including less estrogen rise and acne.
Testosterone creams work in a similar way to gels. Some compounded testosterone creams are used when commercially available options are not appropriate. Skin irritation at the application site is one of the more commonly reported side effects with transdermal testosterone, and patch users should rotate application sites to reduce irritation.
Oral Testosterone
For many years, oral testosterone was not a practical option. Older formulations caused significant liver toxicity. Newer oral testosterone undecanoate formulations have addressed this problem.
A phase 3 randomized controlled trial published in Andrology found that oral testosterone undecanoate brought 87.4% of hypogonadal men into the normal testosterone range after dose titration. No deaths or treatment-related serious adverse events were reported. Improvements in libido, sexual frequency, and mental health scores were also observed.
A two-year clinical analysis published in the Journal of Sexual Medicine confirmed that the newer oral testosterone undecanoate formulation maintained testosterone levels in the mid-normal range over 24 months. Sexual function improved significantly, and no clinically meaningful changes in liver function were found.
Oral testosterone is taken twice daily with food. The fat content of a meal affects absorption, so eating consistently helps maintain steady blood levels. It does not carry the liver toxicity risk of older oral androgens because it is absorbed through the lymphatic system rather than directly through the liver, but it can affect blood pressure, so dosing and follow-up should be monitored by a doctor.
Nasal Testosterone Gel
Nasal testosterone gel is applied inside the nostrils using a small applicator. It is used three times daily, roughly every six to eight hours.
The nasal route allows rapid absorption without the skin contact transfer risk associated with topical gels. Because it is not applied to the skin, there is no concern about hormone exposure to partners or children.
Nasal gel produces faster fluctuations in testosterone levels throughout the day compared to longer-acting formulations. Some men adjust well to this pattern. Others prefer the steadier levels produced by weekly injections or daily skin gels.
Nasal irritation and congestion are the most commonly reported side effects with this formulation. Natesto is the only FDA-approved intranasal testosterone gel currently available in the United States.
Subdermal Pellets
Testosterone pellets are small implants inserted under the skin, usually near the hip or buttocks, through a minor in-office procedure. They release testosterone gradually over three to six months before replacement is needed.
Pellets offer one of the most consistent delivery profiles available. Blood levels remain relatively stable throughout the implant period without the peaks and troughs that can occur with injections or daily gels.
The procedure carries a small risk of infection, pellet extrusion, or bleeding at the insertion site. Once implanted, dose adjustment is not possible until the next insertion cycle. This requires careful pre-procedure planning with a licensed provider.
Summary Table: All Forms of Testosterone Therapy
The table below compares each formulation across frequency, absorption rate, onset of action, and practical considerations to help you understand what sets each option apart.
| Formulation | Frequency | Absorption Rate | Onset of Action | Needle-Free | Transfer Risk | Key Consideration |
| Injectable Testosterone (Cypionate, Enanthate, Undecanoate, Propionate) | Every 2 to 3 days up to every 10 weeks depending on type | Moderate to slow. Released gradually from muscle or subcutaneous depot. | 2 to 4 weeks for most types. Propionate acts faster. Undecanoate stabilizes after the third dose. | No | No | Most widely used. Flexible dosing. Cost-effective. See injectable comparison table above for individual type differences. |
| Testosterone Gel or Cream | Daily | Moderate. Absorbed through skin over 24 hours with daily application. | 3 to 6 weeks for consistent symptom improvement. | Yes | Yes | Needle-free and discreet. Skin contact transfer risk requires care around partners and children. |
| Oral Testosterone Undecanoate | Twice daily | Moderate. Absorbed via lymphatic system. Food intake affects absorption rate. | 3 to 5 weeks for consistent improvement. Steady levels with twice-daily dosing. | Yes | No | No liver toxicity with current FDA-approved formulations. Must be taken with food. |
| Nasal Testosterone Gel | 3 times daily | Fast. Rapidly absorbed through nasal mucosa within hours of each dose. | 1 to 2 weeks for initial response. Levels fluctuate throughout the day. | Yes | No | Fastest non-injectable absorption. No transfer risk. Three-times-daily routine required. |
| Subdermal Pellets | Every 3 to 6 months | Slow and steady. Continuous release from implanted pellets with minimal fluctuation. | 3 to 6 weeks for full effect as the pellet begins releasing consistently. | No (minor procedure) | No | Most stable blood levels of all formulations. Dose cannot be changed after implantation. |
Which Type of Testosterone Is Right for You?
Use this quick framework:
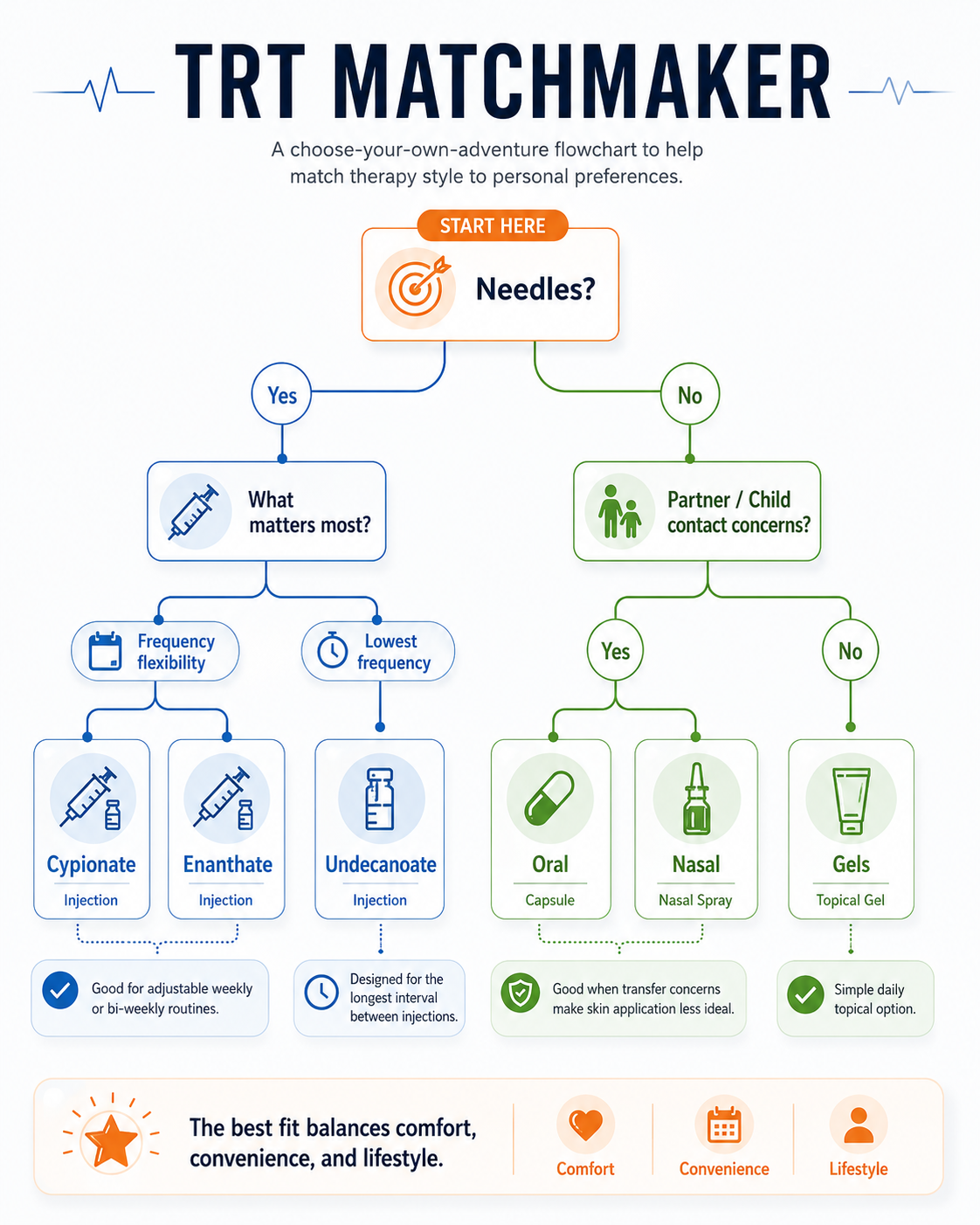
→ Want to avoid needles entirely? Gels, creams, oral, or nasal.
→ Comfortable with injections and want the lowest cost? Cypionate or enanthate.
→ Want injections but minimum frequency? Testosterone undecanoate (every 10 weeks, clinic only).
→ Want maximum stability with no weekly effort? Subdermal pellets.
→ No transfer risk and don't mind three daily doses? Nasal gel (Natesto).
The right formulation depends on your lifestyle, how often you are willing to dose, whether you are comfortable with injections, and which symptoms, medical conditions, or health conditions may affect suitability. Here is a direct breakdown of each option.
Injectable Testosterone: Best for Flexibility and Cost
Injectable testosterone is the most widely prescribed form of TRT. These testosterone injectables are commonly chosen for the dosing flexibility and other benefits they offer. Testosterone cypionate and testosterone enanthate are both cost-effective, self-injectable at home, and allow your provider to adjust dosing based on your blood levels.
Testosterone cypionate has a longer half-life and needs fewer injections per week. Testosterone enanthate has a slightly shorter half-life and may suit men who prefer weekly dosing. Both are available as subcutaneous injections, which most patients find straightforward to manage.
Testosterone propionate requires injections every two to three days. This level of frequency makes it a less practical choice for most men today.
Injectable Testosterone Undecanoate: Best for Lowest Frequency
One injection every ten weeks after loading. This is the lowest-frequency injectable available. It must be given by a healthcare provider in a clinic and requires 30 minutes of monitoring after each dose. Good option for men who want minimal dosing with clinical oversight.
Testosterone Gels and Creams: Best for Avoiding Needles
Applied daily to the skin on the upper arms or shoulders. No injections required, which adds convenience for men who want to avoid needles. Skin contact transfer is a real consideration. The application site must be dry and covered before any physical contact with a partner or child.
The most commonly prescribed testosterone gels in the United States include AndroGel (1% and 1.62%), Testim, and Vogelxo. Compounded testosterone creams are also used when commercially available options are not appropriate for a specific patient.
Oral Testosterone: Best for a Discreet Daily Routine
Taken twice daily with food. No needles, no skin transfer risk. Absorbed through the lymphatic system, not the liver, so it does not carry the liver toxicity risk of older oral formulations. This medication still requires monitoring by a doctor. Consistent meal timing matters for stable blood levels.
Subdermal Pellets: Best for Hands-Off Consistency
Inserted under the skin every three to six months through a minor in-office procedure. Blood levels stay highly stable with no daily or weekly effort required. The dose cannot be adjusted after implantation, so pre-procedure planning with your provider is important.
Nasal Testosterone Gel: Best for No Transfer Risk With Fast Absorption
Applied inside the nostrils three times daily. Absorbs quickly and carries no skin contact transfer risk. Blood levels fluctuate more throughout the day compared to other formulations. Best suited for men who need fast absorption and live with young children or sensitive partners.
Cost and Insurance Context
Cost varies significantly between formulations and matters for long-term adherence. As a general framework:
Injectable testosterone (cypionate, enanthate): Most cost-effective. Both are widely available as generics, typically $30-$100/month depending on dose and pharmacy. Usually covered by insurance for confirmed hypogonadism.
Testosterone gels and creams: Higher cost than injectables at retail. Brand versions (AndroGel, Testim) can exceed $400/month without insurance; generics are more affordable. Often covered under formulary plans.
Oral testosterone undecanoate (Jatenzo, Tlando, Kyzatrex): Premium cost, typically $500+/month without coverage. Insurance coverage varies by plan and diagnosis documentation.
Nasal testosterone gel (Natesto): Higher cost than injectables. Check formulary coverage before prescribing.
Testosterone pellets: Typically $500-$1,000 per insertion procedure, every 3–6 months. Often not covered by insurance and paid out-of-pocket. Total annual cost can exceed injectable or gel options.
Always verify with your insurance provider and compare pharmacy pricing before committing to a formulation.
Risks to Know Before Starting Testosterone Therapy
Testosterone replacement therapy TRT is a medical treatment. Like all medical treatments, it carries risks that are important to understand before starting.
The TestES evidence synthesis published in Health Technology Assessment, which analyzed 35 trials and over 5,600 men, found no significant difference in cardiovascular or cerebrovascular events between TRT and placebo groups in the short to medium term. TRT improved quality of life and sexual function across almost all patient groups studied. Even with reassuring trial data, cardiovascular safety still needs individual risk assessment and ongoing monitoring. That discussion should include prior cardiovascular history, including heart attacks.
Key risks to discuss with your healthcare provider include:
Elevated hematocrit: Testosterone stimulates red blood cell production. If levels rise too high, blood thickens and clotting risk increases. Regular blood tests catch this early.
Fertility suppression: TRT reduces sperm production by suppressing the hormonal signals from the brain. Men who plan to conceive should raise this with their provider before starting treatment.
Estrogen conversion: Some testosterone converts to estrogen through aromatization. This can cause mood swings, water retention, and breast tissue sensitivity if not monitored.
Acne, sleep apnea, and prostate monitoring: Acne can worsen in some men early in treatment. Existing sleep apnea may be affected. PSA and prostate health are tracked throughout therapy. Research does not show that TRT causes prostate cancer, though monitoring remains standard practice.
Most of these risks are manageable with proper monitoring. The increased risk comes from unmonitored or unsupervised use, not from well-managed clinical treatment.
Inject users should test at trough (just before next injection) for the most accurate picture of their baseline levels. Gel users should test 2-4 hours after application.
How Testosterone Deficiency Is Diagnosed
Testosterone replacement therapy is only appropriate for men with confirmed testosterone deficiency. Symptoms alone are not enough.
The standard evaluation includes:
- Total testosterone: Measured via blood test in the morning between 7 and 10 AM, when levels are naturally at their highest. Total testosterone includes free, albumin-bound, and SHBG-bound testosterone. A result below 300 ng/dL is generally considered low, though reference ranges vary by laboratory.
- Repeat testing: At least two separate morning tests on different days are required to confirm low testosterone. A single result is not enough for diagnosis.
- Free testosterone: Measures the biologically active testosterone available for use by the body. It accounts for about 2% to 3% of total testosterone and is the most active form because it can enter cells and trigger cellular functions. Useful when total testosterone is borderline or symptoms persist despite normal total levels.
- LH and FSH: These pituitary hormones help identify the underlying cause of low testosterone.
- SHBG: Sex hormone-binding globulin affects how much testosterone is biologically available. SHBG-bound testosterone accounts for about 40% to 50% of total testosterone and is biologically inactive, acting as a metabolic buffer.
Low testosterone is a clinical diagnosis. It requires confirmed low testosterone levels along with symptoms that affect daily quality of life and helps clinicians assess possible hormonal imbalances.
Monitoring Schedule After Starting TRT
Clinical guidelines recommend blood testing at the following intervals after starting TRT:
- Baseline: Total testosterone, free testosterone, hematocrit, PSA, LH/FSH, lipid panel.
- 3 months after starting: Total testosterone (trough level for injections, peak-plus-trough for pellets), hematocrit, and PSA.
- 6-12 months: Full panel. Ongoing annually or per provider's clinical judgment once stable.
FAQ
What is the most common type of testosterone used in TRT?
Testosterone cypionate is the most commonly prescribed form in the United States. It is cost-effective, widely available, and can be self-administered at home after proper training.
Testosterone Pellets vs Injections: What's the Difference?
Testosterone pellets offer long-term convenience with dosing every 3 to 6 months, while injections provide greater flexibility and easier dose adjustments. Pellets maintain steady levels but require a minor procedure, whereas injections allow treatment to be fine-tuned based on symptoms and lab results.
What is the difference between testosterone cypionate and testosterone enanthate?
Both are injectable testosterone esters with similar effectiveness. Testosterone cypionate has a slightly longer half-life, which allows more flexibility in dosing intervals. Testosterone enanthate has a slightly shorter half-life and may need more frequent injections for stable blood levels.
Is oral testosterone safe for the liver?
Newer oral testosterone undecanoate formulations are absorbed through the lymphatic system rather than directly through the liver. Clinical trials have not found clinically significant changes in liver function with these newer formulations. Oral testosterone may also require monitoring for blood pressure.
What are subcutaneous injections?
Subcutaneous injections are given into the fat layer just beneath the skin, rather than deep into muscle. They are used with testosterone cypionate and enanthate, and research suggests they can produce more stable blood levels than intramuscular injections for some patients.
Can I switch between formulations?
Yes, but changes should always be made with a licensed healthcare provider or doctor. Dose adjustments are often needed when switching, and blood levels should be monitored after any change.
Do all testosterone types carry the same risks?
Most core risks apply across all formulations. These include elevated hematocrit, fertility suppression, estrogen conversion, and prostate monitoring. Some risks are specific to certain products. Injectable testosterone undecanoate carries a rare pulmonary oil microembolism risk. Transdermal gels carry a skin contact transfer risk.
How long does it take to feel results from testosterone therapy?
Response times vary by formulation and by person. Some men notice improvements in energy and mood within a few weeks. Sexual function improvements often take longer, typically one to three months. Full assessment of treatment response is usually done after three to six months of consistent therapy.
Conclusion
Different types of testosterone work differently in the body. Each has its own dosing schedule, delivery method, and risk profile. Injectable testosterone, particularly testosterone cypionate, remains the most widely used option. Its effectiveness, flexible dosing schedule, and lower cost make it a practical choice for most men with confirmed testosterone deficiency.
Oral testosterone and transdermal gels offer needle-free alternatives supported by strong clinical evidence. Longer-acting injectable options reduce the burden of frequent dosing for men who qualify. No single form is right for everyone.
Proper blood testing comes first. Treatment decisions follow from that, guided by a licensed healthcare provider who understands your health history, lifestyle, and goals.
Disclaimer
This content is for educational purposes only and does not replace medical advice. Testosterone therapy and hormone-related decisions should be guided by a licensed healthcare provider.
References
Barbonetti A, D'Andrea S, Francavilla S. Testosterone replacement therapy. Andrology. 2020;8(6):1551-1566. doi:10.1111/andr.12774. PMID: 32068334. https://pubmed.ncbi.nlm.nih.gov/32068334/
Shoskes JJ, Wilson MK, Spinner ML. Pharmacology of testosterone replacement therapy preparations. Transl Androl Urol. 2016;5(6):834-843. doi:10.21037/tau.2016.07.10. PMID: 28078214. PMCID: PMC5182226. https://pubmed.ncbi.nlm.nih.gov/28078214/
Miner M, Wang C, Kaminetsky J, et al. Safety, efficacy, and pharmacokinetics of oral testosterone undecanoate in males with hypogonadism. Andrology. 2024;13(4):882-893. doi:10.1111/andr.13747. PMID: 39252657. https://pubmed.ncbi.nlm.nih.gov/39252657/
Honig S, Gittelman M, Kaminetsky J, et al. Two-year analysis of a new oral testosterone undecanoate formulation in hypogonadal men: efficacy, impact on psychosexual function, and safety. J Sex Med. 2022;19(12):1750-1758. doi:10.1016/j.jsxm.2022.09.002. PMID: 36272969. https://pubmed.ncbi.nlm.nih.gov/36272969/
Cruickshank M, Hudson J, Hernandez R, et al. The effects and safety of testosterone replacement therapy for men with hypogonadism: the TestES evidence synthesis and economic evaluation. Health Technol Assess. 2024;28(43):1-210. doi:10.3310/JRYT3981. PMID: 39248210. PMCID: PMC11404359. https://pubmed.ncbi.nlm.nih.gov/39248210/