You are tired all the time. Your motivation has dropped. You feel like a different person than you were five years ago. If that sounds familiar, stress and your hormones may have more to do with it than you think.
Cortisol and testosterone work against each other in the body. When cortisol goes up, testosterone often goes down. The relationship is not perfectly one-to-one, but the pattern is well established in the research.
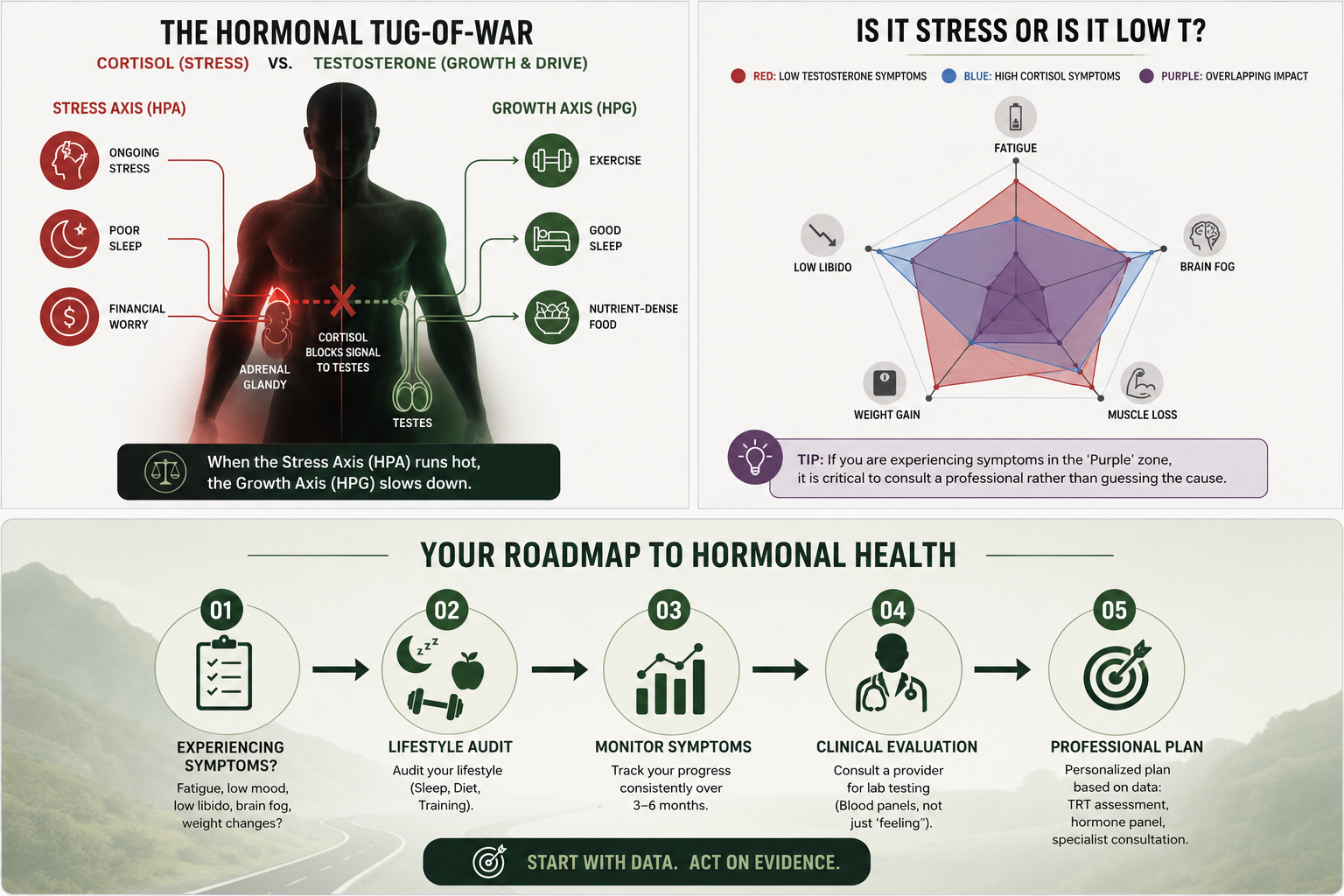
This matters because long-term stress is common. Work pressure, poor sleep, and financial worry all keep cortisol levels high. Over time, that can chip away at testosterone levels and produce symptoms that many men write off as just getting older.
This article explains the cortisol vs. testosterone relationship, what happens when that balance breaks down, and what the evidence actually supports when it comes to addressing it.
What Is Cortisol and What Does It Do?
Cortisol is your primary stress hormone. Your body releases it when it senses danger or pressure. It is produced by the adrenal glands and controlled by the HPA axis, which stands for the hypothalamic-pituitary-adrenal axis.
Here is how it works. Your brain detects a stressor. The hypothalamus sends a signal. The pituitary picks it up and tells the adrenal glands to release cortisol. The whole process can kick off within minutes.
In small doses, cortisol is helpful. It raises your blood sugar, sharpens focus, and helps you respond quickly. The problem starts when it stays elevated for a long time.
What Is Testosterone and How Is It Produced?
Testosterone is the main male sex hormone. In men, it is mostly made in the testes. A smaller amount comes from the adrenal glands. Its production is controlled by the HPG axis, the hypothalamic-pituitary-gonadal axis.
The process works like this. The hypothalamus releases a signal hormone called GnRH. That tells the pituitary to release LH and FSH. LH then tells the Leydig cells in the testes to make testosterone. Levels are highest in the morning and drop through the day.
Testosterone affects muscle mass, bone strength, libido, mood, energy, and red blood cell production. When several of these start declining at once, low testosterone may be a factor.
How Cortisol and Testosterone Interact: The HPA-HPG Axis Relationship
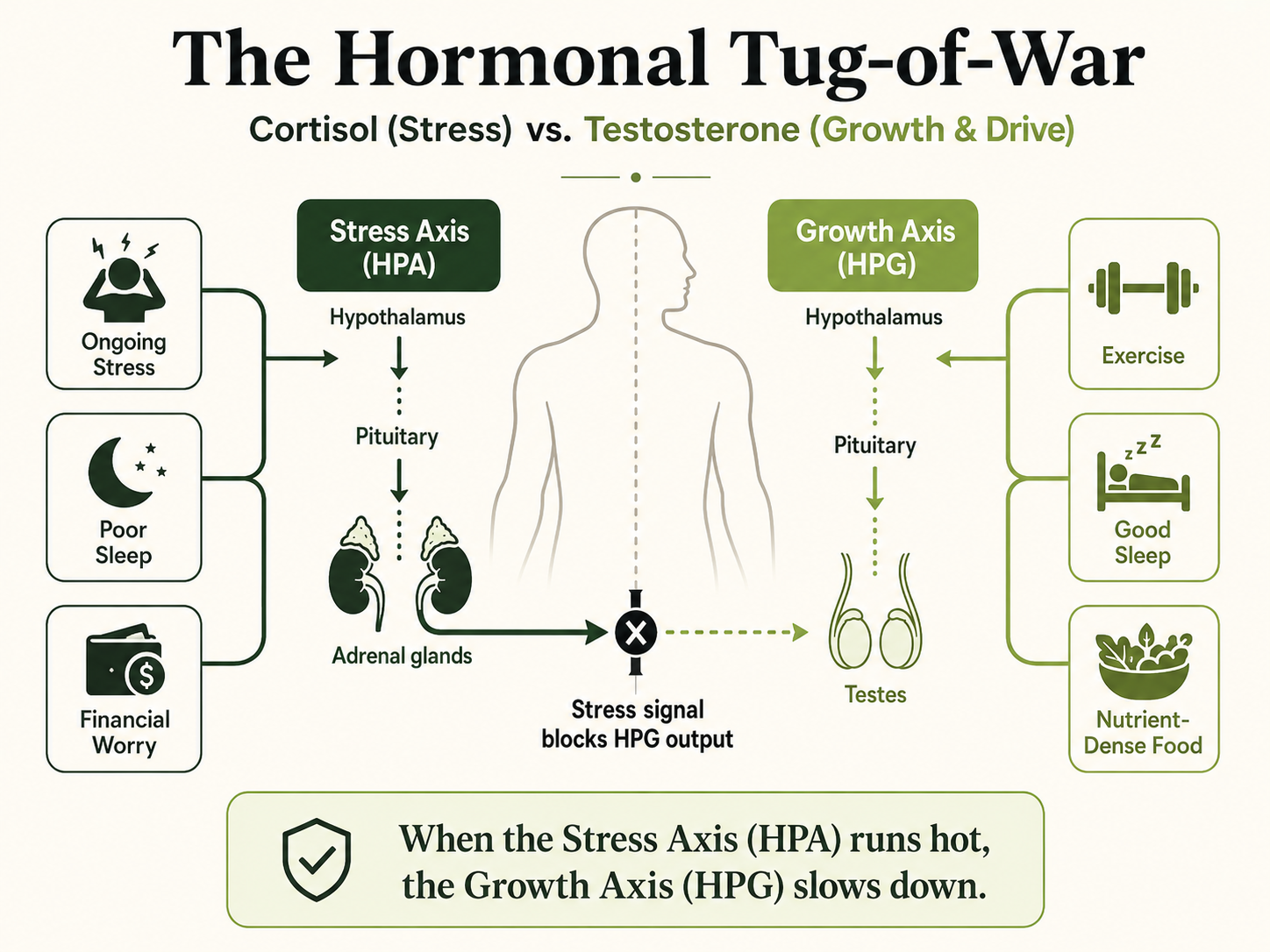
These two hormones are controlled by separate systems in the body and have different roles, even though those regulatory systems talk to each other. When the stress response activates and cortisol goes up, it directly interferes with testosterone secretion.
A review published in Metabolic Brain Disease looked at how the HPA and HPG axes interact. The authors found that long-term activation of the stress axis can reduce testosterone output over time.
High Cortisol Levels and Testosterone Suppression
High cortisol levels suppress testosterone through a few key pathways as part of the body's response to ongoing stress, and this effect can be triggered through these same mechanisms. First, cortisol acts on the Leydig cells and makes them less responsive to LH. Second, it raises a protein called SHBG, which grabs onto free testosterone and takes it out of circulation. This matters clinically: a total testosterone reading may appear within normal range in a chronically stressed man while free testosterone the biologically active fraction is meaningfully suppressed by elevated SHBG. This is why providers should measure free testosterone alongside total testosterone in men presenting with stress-related symptoms.
A study in the Journal of Sports Science and Medicine tested 45 men at rest and after hard exercise. At rest, cortisol and testosterone were not clearly related. After exercise, higher cortisol went with lower total testosterone. The authors noted the link was associative, not proven cause and effect.
A 2025 review in the Indian Journal of Endocrinology and Metabolism looked at the testosterone-to-cortisol ratio as a practical tool. A falling ratio can signal that stress is outpacing recovery.
Shared Precursor Competition (Pregnenolone Steal): Both cortisol and testosterone are synthesized from the same cholesterol-derived precursor pregnenolone. Under chronic stress conditions, the body shunts pregnenolone toward cortisol production, potentially reducing the raw material available for testosterone synthesis. This mechanism is sometimes called the "pregnenolone steal" in clinical endocrinology and provides a biochemical explanation for why men under prolonged physical or psychological stress can experience suppressed testosterone even when LH signaling is intact. It is distinct from the LH suppression pathway and represents a second independent route by which high cortisol can reduce testosterone output.
Acute Stress vs. Chronic Elevated Cortisol
Acute stress is part of the body’s fight or flight mode, and a short, intense stressor may cause a brief rise in testosterone. But that effect is inconsistent and not seen across all studies.
Chronic stress is a different picture. In most cases, a short stress reaction does not have the same hormonal effect as sustained elevation. A study in the journal Stress collected saliva samples from men and women before and after a social stress test. Testosterone dropped in both groups after the stressor. Levels hit their lowest point around 20 minutes in. They had not returned to baseline by the end of the 35-minute window.
The authors also found that the testosterone drop was largely independent of cortisol levels. This suggests the HPG axis responds to stress on its own, not just through cortisol.
When Hormones Fall Out of Balance: What It Actually Feels Like
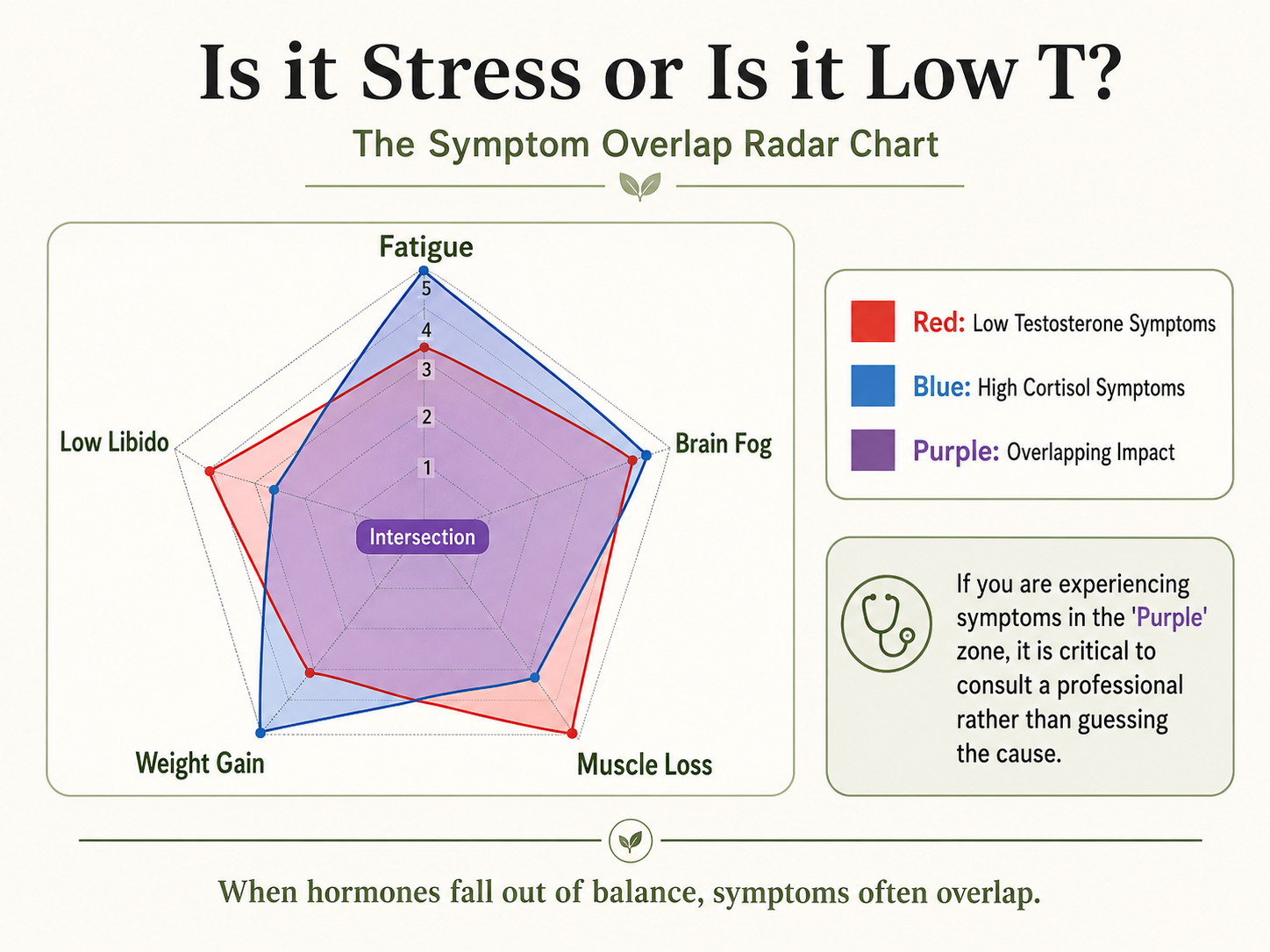
When cortisol stays high and testosterone stays low, it shows up in the body. High testosterone levels support energy, mood, and drive. Low testosterone levels do the opposite. It is not just a number on a lab report. Most men feel it in their daily life before they ever get tested.
A clinical review in Medical Clinics of North America listed the main symptoms of low testosterone as reduced libido, erectile difficulty, muscle loss, increased body fat, low bone mass, depressed mood, and fatigue. A review in Urologic Clinics of North America also noted strong links between low testosterone, obesity, and metabolic problems.
Here is what that can look like day to day:
Muscle Breakdown
Testosterone drives muscle protein synthesis. When it falls and cortisol stays high, the body shifts into a breakdown state. Strength drops. Recovery slows. Men often notice this even when they are still training regularly.
Mood Changes
Low testosterone has been linked to depressive feelings, irritability, low motivation, emotional flatness, and anxiety. The connection between testosterone and mood is real. But it is not the only factor at play. Multiple systems are involved.
Decreased Sexual Function
Reduced libido and erectile difficulty are two of the most commonly reported symptoms of low testosterone. Testosterone plays a role in both desire and physical response. Other factors like stress, cardiovascular health, and medications also contribute.
TRT is FDA-approved for testosterone deficiency treatment, not for men without clinically confirmed hypogonadism. It can be given by injections, gels, or pellets, and potential adverse effects include acne and prostate enlargement.
Low Energy Levels
Fatigue and low drive are common with low testosterone. High cortisol makes this worse. It disrupts sleep and interferes with how the body regulates energy. The two together can leave a man feeling consistently drained.
Poor Cognitive Function
Evidence suggests testosterone plays a role in memory, focus, and mental sharpness. The review in Urologic Clinics of North America found that men with low androgens showed signs of cognitive decline. The evidence here is moderate. Results vary from person to person.
This use has not been approved by the FDA.
Low Bone Density
Testosterone helps maintain bone strength throughout a man's life. When levels fall for a long time, bones get weaker. This raises the risk of fractures and osteoporosis. It is one of the most overlooked effects of long-term low testosterone.
Weight Gain
Low testosterone is linked to higher body fat, especially around the belly. That fat tissue converts testosterone to estrogen through a process called aromatization. The result is a cycle: lower testosterone leads to more body fat, which drives testosterone even lower.
The Dual-Hormone Hypothesis: When High Cortisol Blocks Testosterone's Drive
The Core Idea
The dual-hormone hypothesis says cortisol and testosterone play different roles in behavior, and testosterone is more likely to lead to dominance-related behavior when cortisol is low. When cortisol is high, testosterone's influence on status-seeking behavior, dominance, and drive is blocked or reversed.
The idea was first tested in research published in Hormones and Behavior. They looked at leadership and competition tasks. Testosterone was linked to dominant behavior, but only in people with low cortisol. In high-cortisol individuals, that link disappeared or flipped.
What the Data Shows
A meta-analysis in Neuroscience and Biobehavioral Reviews pulled together 33 studies with data from over 8,500 people. Here is what they found:
- High cortisol does appear to blunt testosterone's influence on behavior, but the effect across the general population is small
- The interaction showed up most clearly in direct competition and social status situations
- In everyday contexts, the link between the two hormones was weaker
- The researchers flagged that positive findings may have been overrepresented, meaning the true effect could be even smaller
The literature does not show a simple positive association between cortisol and testosterone across everyday settings.
Who It Applies To
A study in Aggressive Behavior found the testosterone-cortisol interaction only mattered in men who were already prone to dominant behavior. This work suggests the hypothesis does not apply the same way to every man. Individual differences matter a lot.
What This Means for You
If you are under high perceived stress, your cortisol is likely elevated. Research suggests that it can blunt the drive and assertiveness that testosterone normally supports. That is not permanent. It is a physiological state that can respond to lifestyle changes and, when needed, medical evaluation to evaluate persistent symptoms and hormone status.
One Test Does Not Tell the Whole Story: Why Perceived Stress Alone Should Not Drive Medical Decisions
Hormone Levels Follow Status, They Do Not Always Predict It
Research in the Journal of Neuroendocrinology studied male cynomolgus monkeys over time. Neither cortisol nor testosterone levels predicted which monkey would become dominant. The dominant monkey only showed higher hormone levels after it had already become dominant. In these males, the hormones reflected where things stood, not where they were headed. That is an important limit to keep in mind when applying animal research to human health decisions. These results align with prior findings that hormone measures often reflect current social position more than future outcomes.
Hormones Fluctuate Constantly
Most studies measure hormones from saliva samples at one point in time. But hormonal levels fluctuate throughout the day. Sleep, food, body weight, and activity all affect the numbers. A single reading only captures a small slice of what is actually happening, not trends across a long period; in research, hair testing is sometimes used to study those patterns over time.
Stress Perception Is Not a Diagnosis
Feeling stressed does not mean your testosterone is low. Many men under heavy, ongoing stress still have testosterone levels in the normal range. Lab testing is the only reliable starting point.
How to Lower Cortisol and Support Testosterone Naturally: What the Evidence Shows
Lifestyle has a direct effect on both hormones. The evidence here is more consistent and more actionable than the cortisol-testosterone relationship on its own.
Sleep matters
Research in the Indian Journal of Endocrinology and Metabolism found the testosterone-to-cortisol ratio drops with sleep loss. Cortisol rises. Testosterone output in the morning falls. Sleep quality directly affects testosterone production.
Research shows that restricting sleep to around 5 hours for one week can reduce daytime testosterone levels by 10-15% in young healthy men. The mechanism is through LH pulsatility - poor or shortened sleep disrupts the hormonal signals that drive morning testosterone production. Most men produce the majority of their daily LH pulses during sleep, particularly during REM stages. Aiming for 7-9 hours supports this process.
Resistance training
Resistance training itself supports testosterone production and helps keep the testosterone-to-cortisol ratio healthy. But overtraining raises cortisol and can suppress testosterone. Recovery is part of the work, not a break from it.
Body weight
Excess belly fat raises estrogen through aromatization and is linked to higher cortisol levels. Weight gain and hormonal imbalance can reinforce each other.