Yes, obesity lowers testosterone. This is one of the most consistently supported findings in men's health research, confirmed across decades of population studies, clinical trials, and mechanistic investigations.
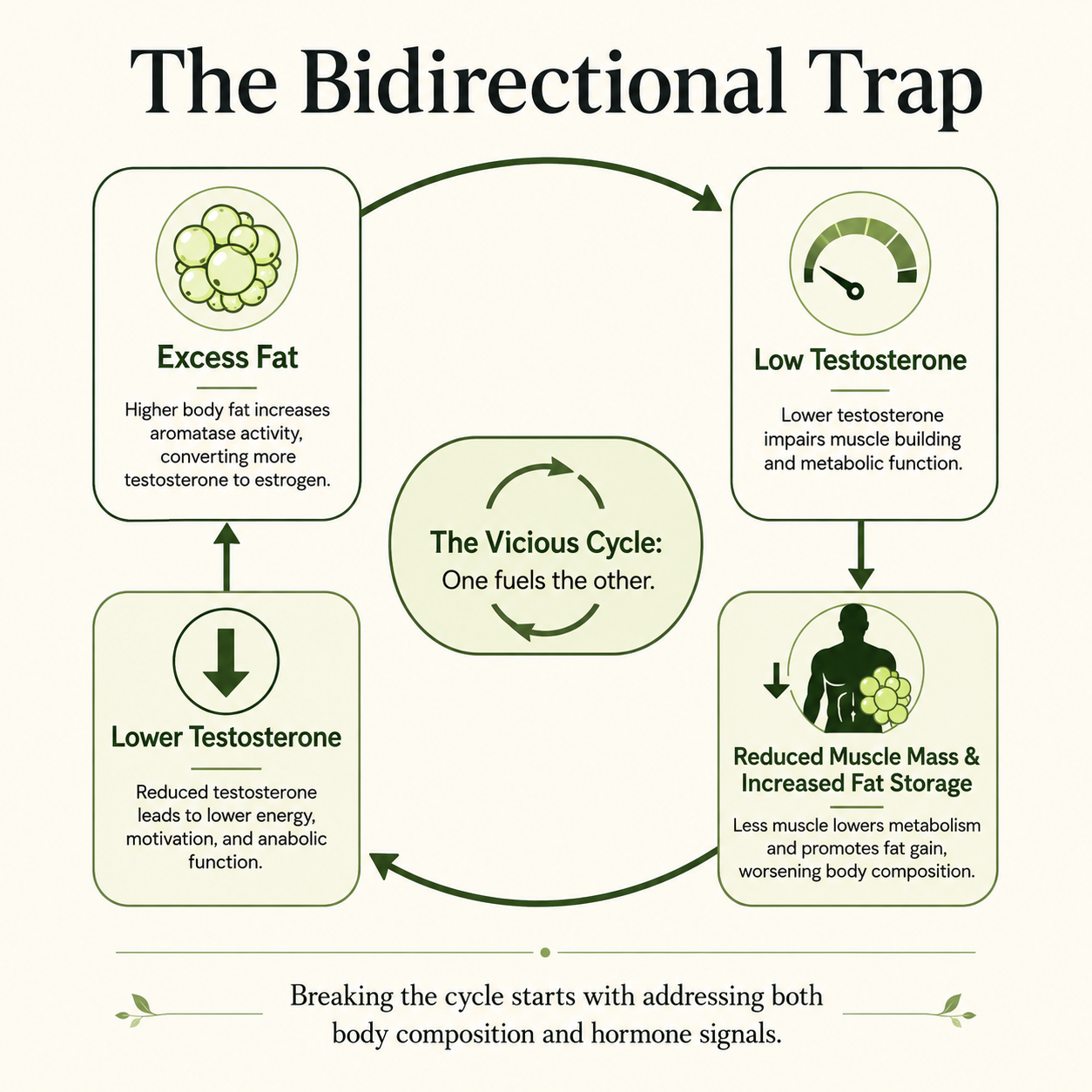
You might already suspect something is off. Persistent fatigue, low libido, mood that feels flat, a waistline that keeps expanding despite reasonable effort. These experiences are common in men carrying excess weight, and the connection to testosterone levels is not a coincidence. Excess body fat actively suppresses the hormonal systems that produce testosterone, while low testosterone independently drives further fat accumulation. If that sounds like a trap, it is. Researchers describe it as a self-perpetuating cycle, and breaking it requires understanding both sides of the equation.
This matters beyond the scale. Testosterone plays a central role in muscle mass, bone density, metabolic health, sexual function, and cardiovascular risk. When obesity pulls testosterone down, the downstream effects touch nearly every system in the body. And when those effects compound over years, the clinical consequences become significant.
This article covers what the research actually shows about the obesity-testosterone link, the biological mechanisms driving it, the longitudinal results on weight loss and hormone recovery, and when testosterone therapy may or may not be an appropriate next step.
Does Obesity Lower Testosterone? What the Body Mass Index Data Shows
Obesity lowers testosterone, and the effect scales with severity. The higher the body mass index, the greater the suppression.
A 30% Reduction in Obese Men
A comprehensive review published in the Asian Journal of Andrology analyzed data from the European Male Aging Study, which followed 3,219 men across multiple countries. The findings were clear: obesity was associated with an 8.7-fold increased risk of secondary hypogonadism compared to normal weight. One study from 2007 found that each one point increase in BMI decreases testosterone by about 2%. Obese men had total testosterone levels approximately 5.9 nmol/L lower than lean men. Overweight men showed lesser but still significant reductions. You may find your own numbers sitting in a range that looks borderline normal on paper but reflects meaningful hormonal suppression when the context of your body weight is factored in.
Obesity Outranks Age as a Predictor of Low T
This is the part most men do not expect. The same review found that epidemiological data identifies obesity as the single most powerful predictor of low testosterone in men, and that it contributes more to age-associated testosterone decline than aging itself, a pattern seen not only in older men but also in young men and one that can carry health consequences into adulthood for adults. Men often blame years when the more accurate explanation is body fat. If you are in your 40s, carrying significant abdominal weight, and experiencing low testosterone symptoms, your waist circumference may be doing more hormonal damage than your birthday.
40% of Obese American Men Have Low Testosterone
A cross-sectional study of 1,849 community-dwelling obese American men found that 40% had low testosterone levels. Men with a body mass index above 35 to 40 showed reductions of more than 50% in both total and free testosterone compared to lean men. You are not an outlier if your levels have dropped significantly. Among obese men, it is the norm.
Why Your Body Fat Is Working Against Your Testosterone
Adipose tissue is not passive storage. It is metabolically active, and in the context of male hormones, it actively works against testosterone production through several compounding mechanisms.
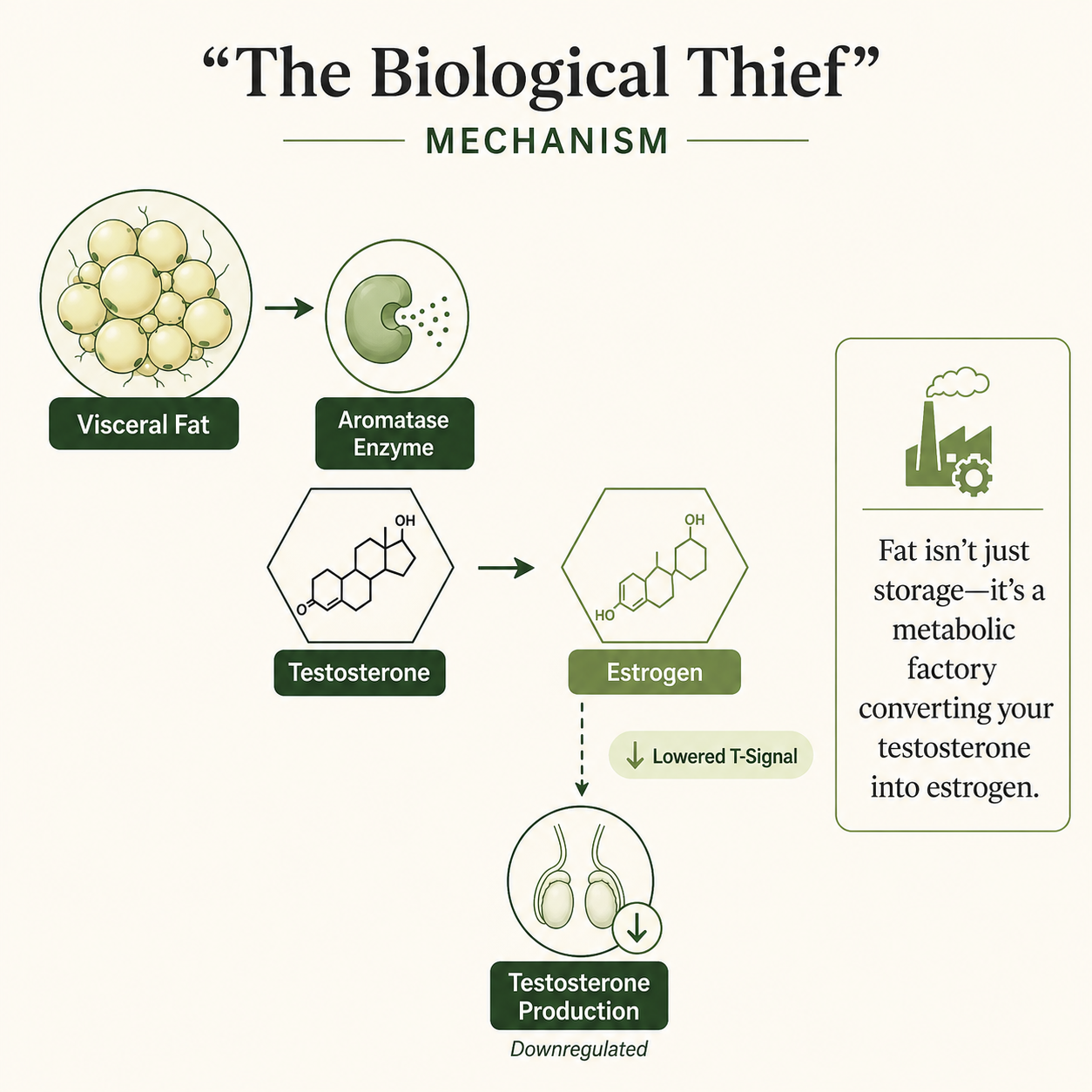
Your Fat Cells Are Quietly Converting Testosterone Into Estrogen
Fat cells, particularly visceral adiposity, express an enzyme called aromatase. Aromatase converts testosterone into estradiol, a form of estrogen. As fat mass increases, aromatase activity rises. More testosterone is diverted into estrogen conversion rather than remaining available as the active male hormone. The resulting increase in estrogen then signals the pituitary gland to reduce luteinizing hormone output. Luteinizing hormone is what tells the testes to produce testosterone. When that signal weakens, testosterone production falls. You lose testosterone at both ends: more is being converted away, and less is being produced.
How Insulin Resistance Steals Your Available Testosterone
Obesity drives insulin resistance, and insulin resistance suppresses the liver's production of sex hormone binding globulin, while low testosterone can further worsen insulin sensitivity. SHBG is the carrier protein that binds testosterone in the bloodstream. Lower SHBG means total testosterone readings drop, even if free testosterone remains temporarily stable. The review in the Asian Journal of Andrology described this as the dominant mechanism in moderate obesity, particularly in younger men. If your total testosterone is low but your provider has not measured SHBG alongside it, the picture of your low free testosterone may be incomplete, and this metabolic disruption can contribute to energy imbalance.
Severe Obesity Shuts Down the Signal That Tells Your Body to Make Testosterone
In more severe obesity, the suppression goes deeper. The hypothalamic-pituitary-testicular axis, the hormonal chain of command that governs testosterone production, becomes functionally impaired. Adipose tissue releases pro-inflammatory cytokines, leptin, and insulin, all of which inhibit this axis at multiple levels. The result is that both luteinizing hormone and testosterone fall together, a pattern called functional hypogonadism; the medical term for this low-testosterone state is hypogonadism when the HPT axis is suppressed by the metabolic environment. It is distinguishable from structural hypogonadism in that the testes themselves are not damaged. The suppression is driven by the metabolic environment, and it can be reversed with sufficient weight loss.
What Actually Happens to Your Testosterone When You Lose Weight
Weight loss raises testosterone. The relationship is proportional: the more weight you lose, the larger the hormonal recovery.
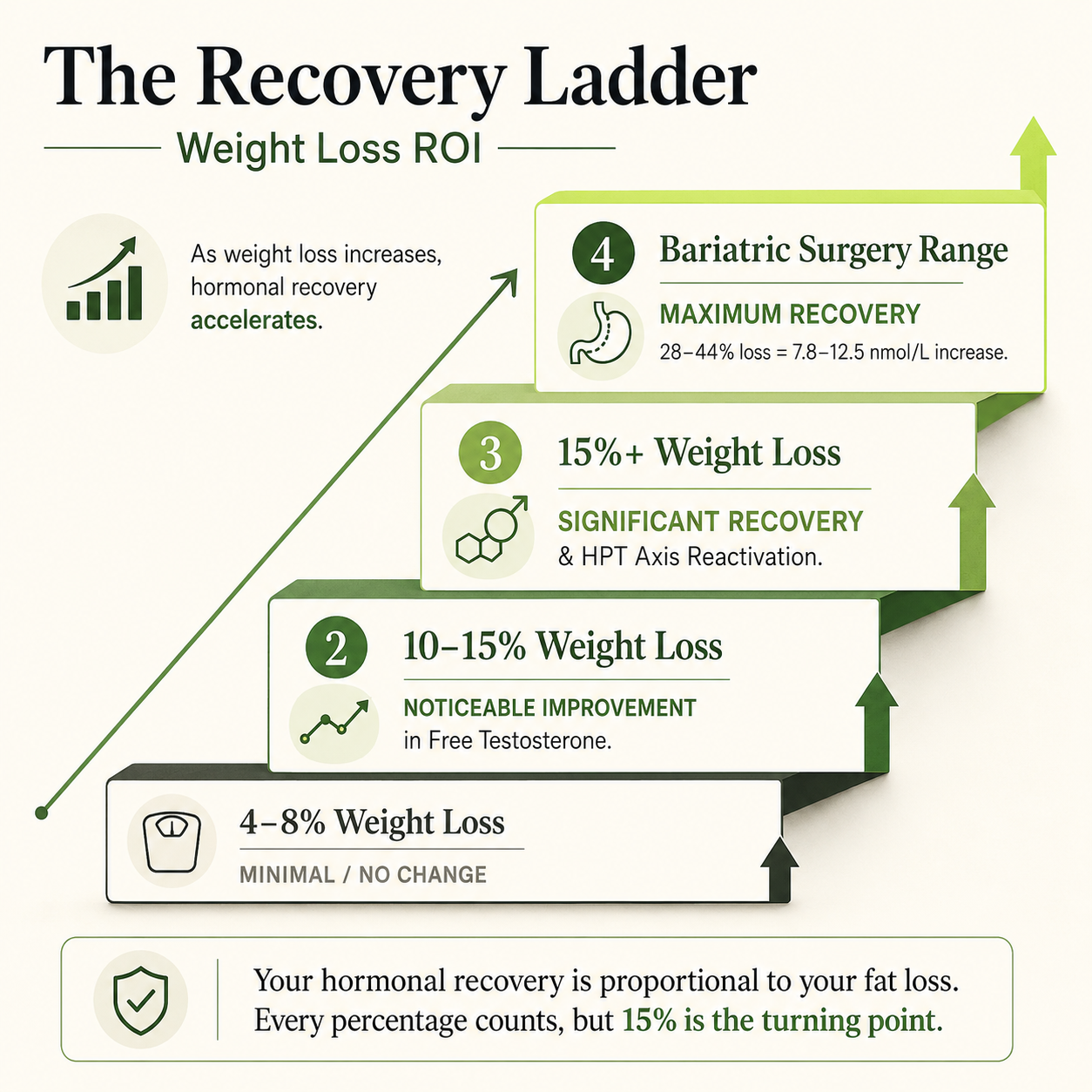
Diet Alone Raises Testosterone, But Only So Much
The same Asian Journal of Andrology review analyzed 15 published trials assessing weight loss interventions and testosterone. Diet-based approaches led to modest weight loss, typically 6 to 17%, and corresponding testosterone increases of 2.9 to 5.1 nmol/L. These gains are meaningful but limited by how much weight most men can realistically lose and sustain through diet alone. Small reductions of 4 to 8% showed minimal or no testosterone improvement across several studies.
Lose Enough Weight and Your Body Starts Producing Testosterone Again
Longitudinal results from the European Male Aging Study showed that minor weight loss produced only modest testosterone increases, likely through SHBG changes. However, weight loss exceeding 15% produced significantly greater total testosterone gains and, critically, increases in free testosterone, showing that larger weight loss is associated with increased levels of testosterone, alongside a rise in luteinizing hormone. That rise in LH indicates genuine reactivation of the hypothalamic-pituitary axis, not just a passive readjustment of binding proteins. Significant weight loss restores the signal chain. This is not a small distinction: it means the testes are receiving the instruction to produce testosterone again.
Bariatric Surgery Produces the Largest and Most Sustained Results
A review published in Gender Medicine evaluated the effects of both surgical and non-surgical weight loss on sex hormones in obese men. Bariatric surgery produced weight loss of 28 to 44% and testosterone increases of 7.8 to 12.5 nmol/L across reviewed studies. Similar results have been reported across multiple surgical studies. These gains substantially exceeded diet-based outcomes. Sexual quality of life improvements were also more consistent with surgical weight loss, including better erectile function. The review described bariatric surgery as the most effective treatment for obesity-related male hypogonadism, with related findings also presented through the American College of Surgeons. If you are considering surgical options, the hormonal implications are among the most well-documented benefits.
What Happens to the Rest of Your Body When This Cycle Goes Unchecked
The effects of this cycle extend well beyond testosterone numbers on a lab report.
Your Blood Sugar, Cholesterol, and Waistline Are All Connected to This
A meta-analysis of 20 observational studies published in PLoS One involving over 10,000 men found that low total testosterone, SHBG, and free testosterone were all independently associated with increased risk of metabolic syndrome. Men in the lowest quartile of testosterone were 1.69 times more likely to have metabolic syndrome than those in the highest quartile. The associations were strongest for hypertriglyceridemia, abdominal obesity, and hyperglycemia. You may have been told your blood sugar or cholesterol numbers are concerning without realizing they are part of the same hormonal picture.
Erectile Dysfunction and Low Libido
A review published in Current Opinion in Endocrinology, Diabetes and Obesity confirmed that testosterone deficiency in obese men contributes to erectile dysfunction, reduced sexual desire, and reduced quality of sexual life. These symptoms are not purely psychological, and they are not inevitable. They are connected to measurable hormonal suppression driven, in part, by excess fat mass. Ongoing testosterone deficiency can also contribute to infertility. If you are experiencing low libido or erectile difficulties alongside weight gain, a blood test for total and free testosterone is a reasonable first clinical step.
Cardiovascular Disease and High Blood Pressure
Abdominal obesity is an independent risk factor for cardiovascular disease, and its hormonal effects compound that risk. Low testosterone is associated with increased fat mass, reduced lean body mass, insulin resistance, hypertension, dyslipidemia, and stroke risk, all of which elevate cardiovascular risk. The bidirectional nature of the obesity-testosterone relationship means that a man gaining visceral weight is simultaneously worsening his metabolic syndrome risk and suppressing the hormone that would otherwise help him counter it. This is why treating the weight, not just the testosterone number, is the clinical priority.
Depression and Energy Levels
Low testosterone in the context of obesity is associated with depressive feelings, reduced motivation, emotional flatness, and persistent fatigue. These mood-specific symptoms are not separate from the metabolic picture. They share the same hormonal substrate. Men with obesity and low testosterone often experience these effects together, and neither resolves fully without addressing both body composition and the underlying hormonal environment.
Why Your Waist Size Tells a Bigger Story Than the Number on Your Scale
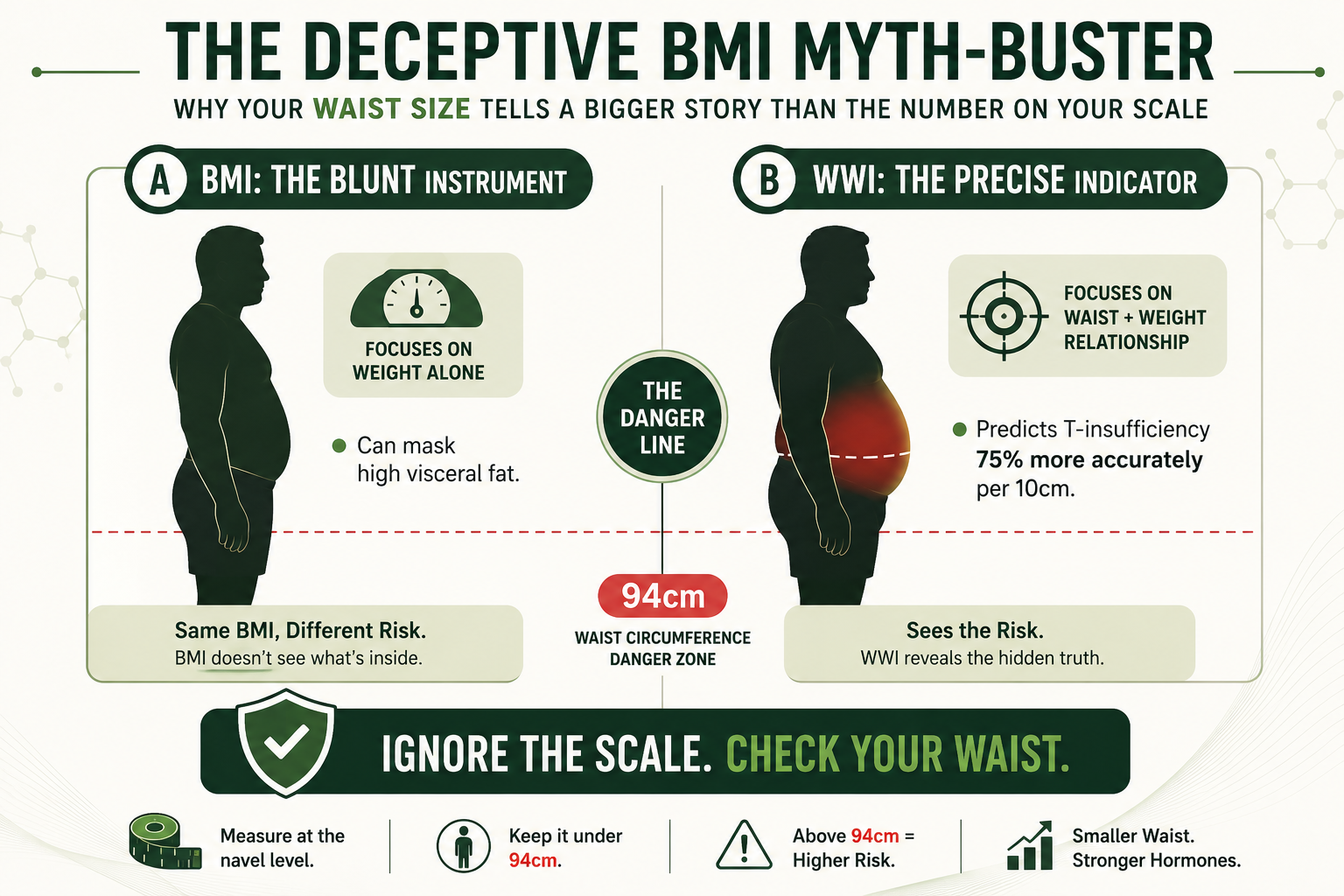
Body mass index is a blunt instrument. Waist circumference and visceral adiposity are more clinically informative when assessing testosterone risk.
A 2008 research of 1,862 men indicated that a four-inch (10 cm) waist circumference increase raised low testosterone risk by 75%. Ten years of ageing only increased probabilities by 36%. Age is less predictive than waist circumference.
Research from the European Male Aging Study found that visceral fat mass, not BMI alone, was more closely linked to testosterone suppression and cardiovascular risk. Men who are "metabolically obese but normal weight," meaning they carry significant visceral fat despite a BMI in the normal range, can experience testosterone suppression equivalent to men who are clinically obese by BMI standards. Conversely, some men with a higher BMI but healthier fat distribution have preserved testosterone levels.
In a 2024 Scientific Reports study, the Weight-Adjusted-Waist Index (WWI) was found to predict testosterone insufficiency better than BMI or standard waist circumference. WWI standardizes waist circumference for body weight and correlates better with cardiometabolic risk and testosterone suppression than other measurements. This measure is increasingly used by obesity-testosterone researchers.
If your waist circumference is above 94 cm, that is where the hormonal risk concentrates. Reducing waist size, not just overall body weight, is associated with the most meaningful testosterone recovery. You may find that shifting your goal from a number on the scale to a reduction in abdominal girth better captures what your hormones actually respond to.
Natural Ways to Support Testosterone Through Weight Management
For men with obesity and low testosterone, lifestyle changes are the first and most important clinical intervention. Testosterone therapy is not a substitute for them.
Resistance Training and Exercise
Resistance training preserves and builds lean body mass, which increases resting metabolic rate and reduces relative fat mass. It also directly stimulates testosterone production through acute hormonal responses to heavy compound exercise. Three to four sessions per week of progressive strength training is one of the most evidence-supported tools available to men working to improve both body composition and hormonal health. You do not need to become a competitive lifter. Consistency over months matters more than intensity at any single session.
Healthy Diet and Losing Weight
A healthy diet that produces sustained caloric deficit is the primary driver of fat loss, and fat loss is what drives testosterone recovery in obese men. Protein adequacy supports lean body mass preservation during weight loss. Reducing ultra-processed foods, refined carbohydrates, and excess sugar reduces the insulin load that suppresses SHBG. No single dietary pattern is uniquely superior, but the degree of weight loss achieved is the best predictor of testosterone improvement, as confirmed across multiple intervention studies. When diet and exercise alone are not enough, weight loss medications may also be considered.
Sleep Quality
Testosterone production is concentrated during deep sleep. Chronic sleep deprivation, or unrecognized sleep apnea, suppresses testosterone production significantly. If you are carrying excess weight and also experiencing daytime fatigue, poor concentration, or your partner has mentioned that you stop breathing during the night, sleep apnea evaluation is warranted before attributing all of your symptoms to testosterone alone. Treating sleep apnea can meaningfully improve testosterone levels independent of weight changes.
Stress and Cortisol Management
Chronically elevated cortisol from psychological or physiological stress suppresses the hypothalamic-pituitary axis. The same axis that obesity disrupts is also sensitive to stress hormones. Sleep, resistance training, and managing workload or psychological stressors all reduce cortisol burden and support the hormonal environment your body needs to produce adequate testosterone.
If meaningful lifestyle changes over several months have not resolved your symptoms, and your body mass index remains above 30, clinical evaluation including morning blood testing for total and free testosterone is an appropriate next step.



