Testosterone and sleep share a bidirectional relationship: poor sleep suppresses testosterone production where one week of five hour sleep can reduce levels by 10–15% while low testosterone disrupts sleep architecture and reduces restorative rest. Testosterone therapy does not act as a direct sleep aid; however, it may indirectly improve sleep for some men by resolving specific issues like night sweats and fatigue. Because sleep apnea can both cause and result from these hormonal imbalances, it is critical to evaluate and treat it before considering hormonal therapy.
Testosterone does not directly improve sleep in the way a sedative or sleep aid would. But if you are asking whether testosterone helps you sleep better, the more accurate answer is that sleep and testosterone affect each other in a bidirectional, clinically important way that many men do not realize.
If you are a man dealing with poor sleep, low energy, fatigue that does not resolve with rest, waking frequently through the night, mood changes, or symptoms that may point to low testosterone, it is worth understanding how closely these two systems are linked. Poor sleep can reduce testosterone production. Low testosterone can worsen sleep quality. When one breaks down, the other often follows.
That connection matters because problems on either side can keep dragging down your rest, energy, and mood unless you address the right cause first. This article explains the biology behind testosterone and sleep, what research shows about testosterone replacement therapy and sleep outcomes, how sleep apnea fits into the picture, and which lifestyle changes may improve both before you consider clinical treatment.
Why Testosterone and Sleep Are More Connected Than Most Men Realize
Testosterone and sleep are not just loosely associated. They are mechanistically linked in ways that run in both directions.
Your Body Makes Most of Its Testosterone While You Sleep
Testosterone production in men follows a circadian pattern that is tightly tied to sleep. A comprehensive review published in Sleep Medicine Reviews by Andersen and Tufik confirmed that nocturnal testosterone is sleep-related, with levels rising during sleep and falling on waking, while circadian effects independent of sleep are minimal.
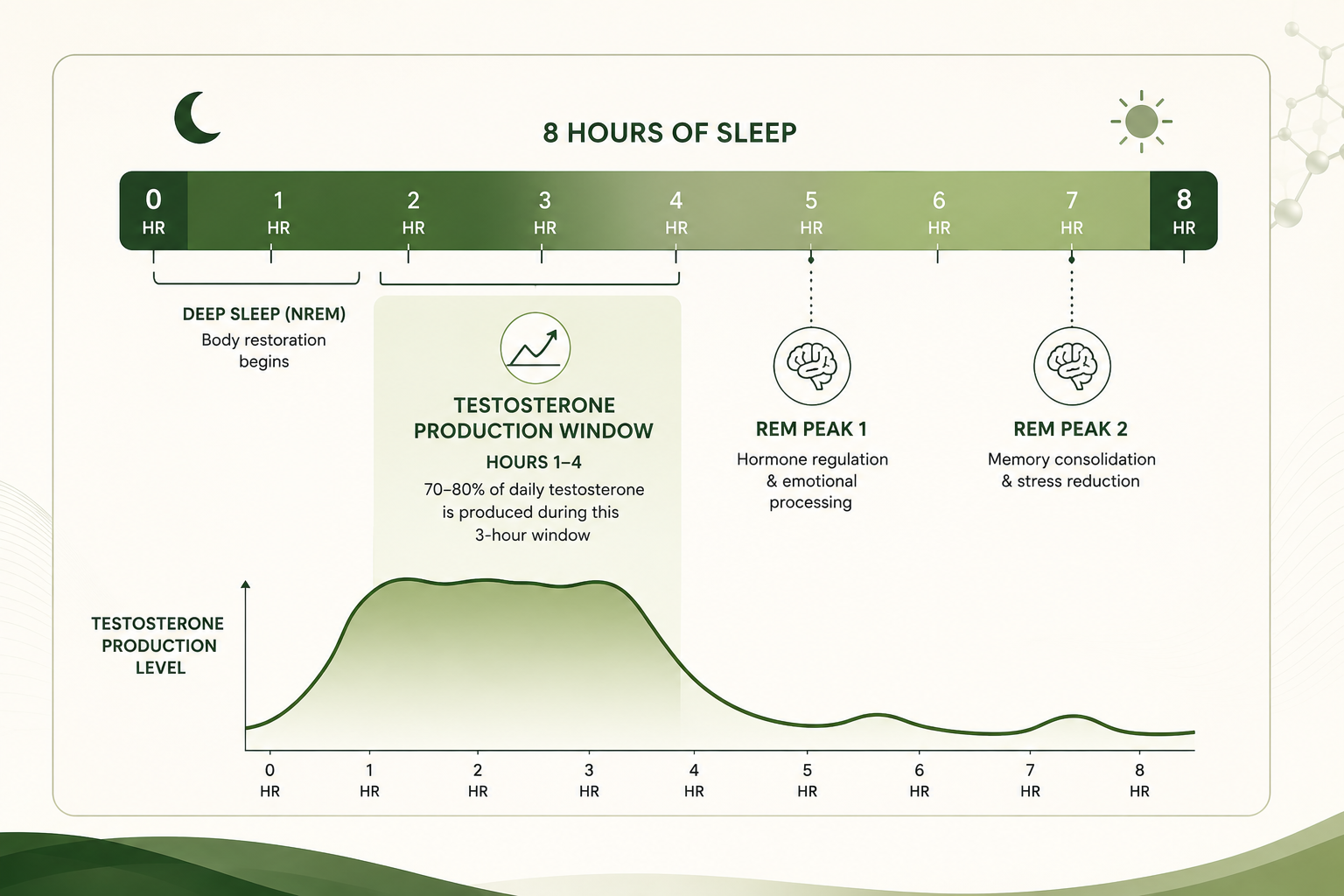
Peak testosterone levels coincide with the onset of REM sleep. When you do not get enough sleep, or when your sleep architecture is disrupted, your testosterone production suffers directly. This is not a small or marginal effect. Sleep is where your body does the hormonal work that keeps your testosterone in a healthy range. You can eat well, train hard, and manage stress, and still suppress your testosterone by consistently sleeping fewer hours per night than your body requires.
The first three hours of uninterrupted sleep represent the critical production window. Research from the Asian Journal of Andrology identifies this early sleep period as when the body generates the hormonal conditions that fuel the overnight testosterone rise. Total fragmentation of sleep architecture, sleep repeatedly broken throughout the night, has been shown to prevent this increase from occurring at all. This is why sleep quality matters as much as sleep quantity: eight hours of fragmented, shallow sleep can fail to produce the testosterone benefits of six hours of deep uninterrupted sleep.
Middle-Aged Men Lose the REM-Testosterone Link Young Men Have
A study published in the Journal of Clinical Endocrinology and Metabolism measured nocturnal testosterone levels in seven middle-aged men and six young healthy men over a 12-hour window with simultaneous sleep recordings. Young men had significantly higher mean testosterone levels at night, higher peak concentrations, and more testosterone pulses. In young men, testosterone rise preceded the first REM sleep episode by 90 minutes in a consistent, coordinated pattern. In middle-aged men, this link between testosterone rhythm and REM sleep was disrupted. The testosterone rise and REM onset were no longer synchronized. If you are a man in your 40s or 50s and you have noticed that your sleep feels less restorative than it used to, this research offers one biological explanation. The hormonal-sleep coordination that supports deep, recovery-oriented sleep begins to break down as testosterone production changes with age.
Losing Sleep Directly Lowers Your Testosterone
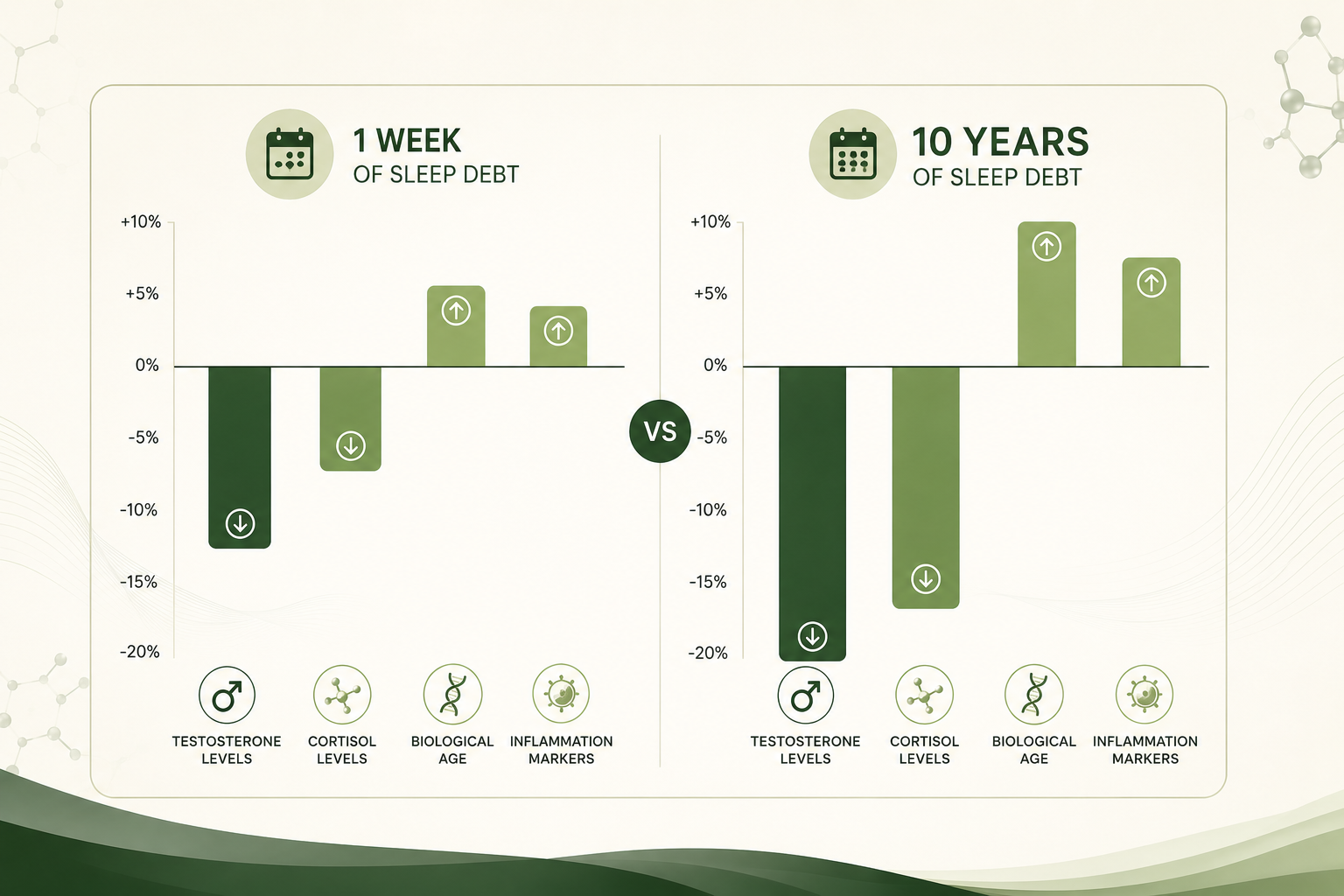
The Sleep Medicine Reviews study by Andersen and Tufik also reviewed experimental data showing that sleep curtailment leads to reduced levels of circulating androgens in healthy men. You do not need severe sleep deprivation for this effect to occur. Consistent sleep restriction, the kind that many men accumulate over years of early starts and late nights, is associated with meaningful reductions in testosterone across the sleep-wake cycle. If you are getting fewer than seven hours per night regularly, your testosterone levels are likely lower than they would be with adequate sleep, and no hormonal intervention fully compensates for that underlying deficit.
The magnitude matters: the JAMA study found that one week of sleeping five hours per night reduced daytime testosterone levels by 10-15% in healthy young men. Normal aging reduces testosterone by roughly 1-2% per year. That means one week of poor sleep produced the hormonal equivalent of 10-15 years of aging. These were not older men or men with pre-existing conditions, they were healthy young adults, which makes the finding applicable across age groups.
Low Testosterone Affects Sleep in These Specific Ways
Low testosterone disrupts sleep through several distinct mechanisms, not all of which are obvious.
Night Sweats and Fragmented Sleep From Hormonal Imbalance
Low testosterone is associated with hormonal imbalance that can trigger night sweats, temperature dysregulation during sleep, and frequent awakenings. These are not the same mechanisms that cause hot flashes in women during menopause, but they involve similar low testosterone and hormone imbalances affecting thermoregulatory control during sleep. If you are waking up damp, kicking off covers repeatedly, lie awake at night, or have difficulty falling asleep before waking in the early morning hours unable to return to sleep, low testosterone may be contributing to that pattern through its effects on hormone balance and the sleep-wake cycle. Nearly 40% of men over age 45 have low testosterone levels.
Reduced Deep Sleep and REM Sleep With Low T
The normal cycle of sleep architecture, including the proportion of time spent in slow-wave deep sleep and REM sleep, as well as healthy sleep cycles, is influenced by testosterone. Low testosterone is associated with reduced restorative rest, less time in the sleep stages that drive physical recovery and hormonal production, poor sleep quality, and worse overall sleep quality. You may be spending enough hours in bed but getting less quality sleep and less of the recovery value that sleep is supposed to deliver.
Persistent Fatigue That Sleep Does Not Fix
One of the most commonly reported symptoms of low testosterone is persistent fatigue that does not resolve after what should have been adequate sleep. This is distinct from simply being tired after a poor night. Men with confirmed testosterone deficiency often describe waking from a full night and still feeling unrefreshed, struggling to build energy through the day, and relying on stimulants to function. This chronic fatigue pattern can reflect the reduced sleep quality described above, or the direct effects of low T on energy metabolism, or both together.
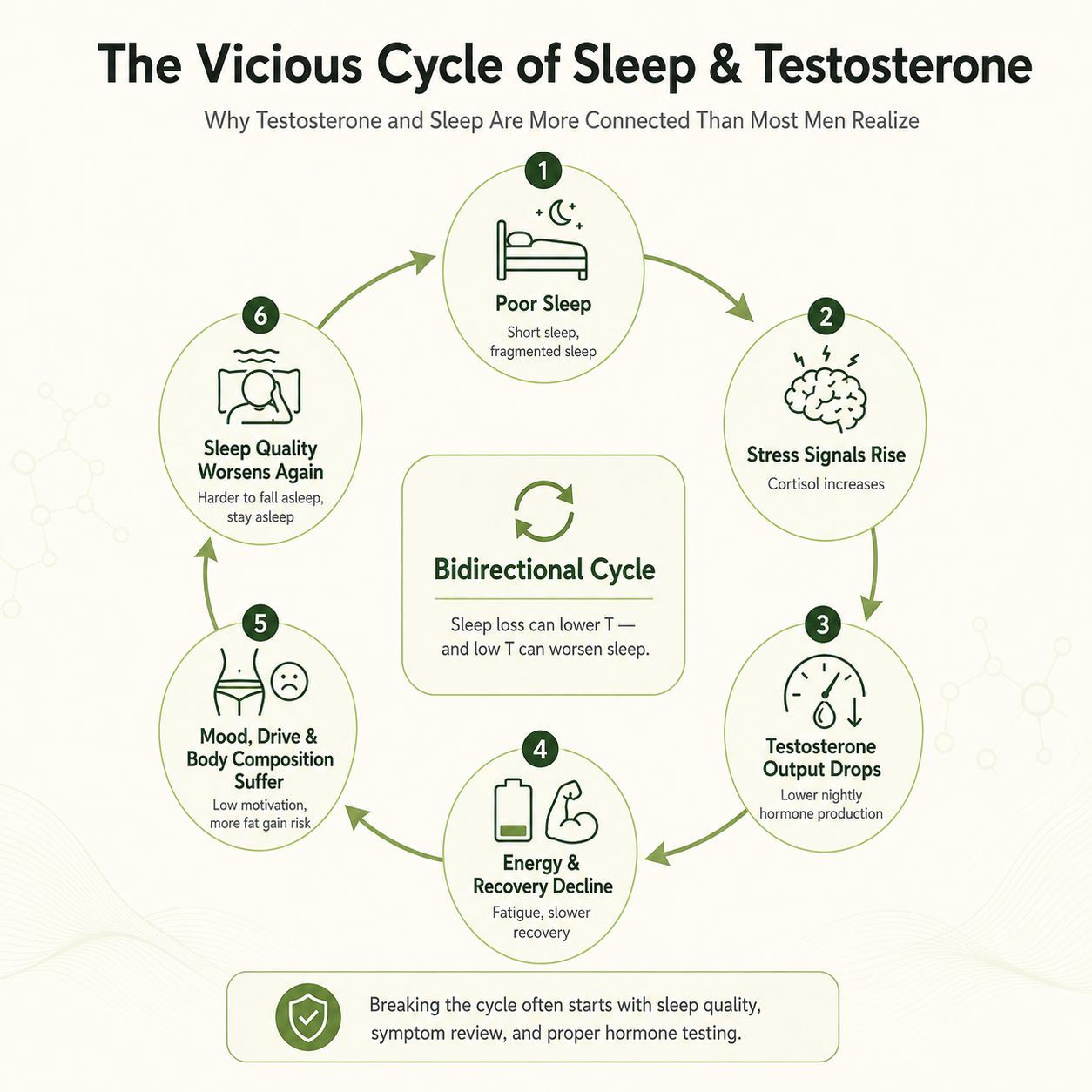
The Self-Reinforcing Loop
Poor sleep and low testosterone create a compounding cycle that does not correct itself without intervention: poor sleep reduces testosterone → lower testosterone reduces sleep quality → disrupted sleep further suppresses testosterone. Simultaneously, poor sleep elevates cortisol, which is an alertness hormone that suppresses testosterone production and makes deeper sleep harder to achieve. Once this cycle is running, each factor reinforces the others. Breaking it typically requires addressing both sleep and hormonal health together rather than treating one in isolation.
What TRT Does and Does Not Do for Sleep Quality
Testosterone replacement therapy may help sleep indirectly by addressing the hormonal causes of night sweats, fragmented sleep, and fatigue. Whether it directly improves sleep quality is a different and more complicated question.
TRT Did Not Improve Sleep Quality in a 14-Week RCT
A randomized controlled trial published in Pain Medicine enrolled 62 men with opioid-induced androgen deficiency and confirmed low testosterone. Participants were randomized to 14 weeks of transdermal testosterone gel or placebo. Mean testosterone levels increased significantly in the treatment group from 223 to 775 ng/dL. Improvements in Insomnia Severity Index scores did not differ significantly between the testosterone and placebo groups. You may find this result counterintuitive if you expected restoring testosterone to significantly improve sleep. The findings suggest that while testosterone replacement corrects the hormonal deficiency, it does not directly resolve insomnia or improve subjective sleep quality in a consistent, measurable way in this population. The causes of sleep disruption in these men may have involved factors beyond testosterone alone.
Where TRT May Help Sleep Indirectly
A systematic review published in Mayo Clinic Proceedings, the critical update of Endocrine Society clinical practice guidelines by Seftel et al., identified trials showing that testosterone therapy produced beneficial effects on sexual function, muscle mass, bone density, and insulin sensitivity in hypogonadal men. While the review noted inconsistent effects on well-being and quality of life, it also acknowledged that some men treated for hypogonadism with severe lower urinary tract symptoms and obstructive sleep apnea showed outcomes that refuted conventional contraindication dogma. Where sleep disruption is driven specifically by low testosterone symptoms, including night sweats and fatigue from hormonal imbalance, restoring testosterone levels may relieve those secondary contributors to poor sleep. The distinction matters: TRT addressing a hormonal cause of sleep disruption is different from TRT directly treating a sleep disorder, though men may still notice more restorative sleep when those secondary symptoms improve.
Sleep Apnea and Testosterone: The Concern That Is Overstated
One of the most commonly cited concerns about testosterone replacement therapy is that it causes or worsens obstructive sleep apnea. The evidence behind this warning is weaker than the frequency with which it appears in clinical guidelines.
The Warning Comes From Small Case Reports, Not Clinical Trials
A review published in the Journal of Sexual Medicine by Hanafy systematically examined the evidence behind cautionary statements linking TRT to obstructive sleep apnea. The review found that the first such caution appeared in 1978 and has since been repeated in clinical literature despite being based on a very small number of case reports. The total number of patients in reports linking TRT to new or worsened sleep apnea was very small relative to the millions of men treated with TRT globally. Findings were inconsistent across reports. The one double-blind placebo-controlled study identified used supraphysiologic doses, far above what is used in standard testosterone replacement therapy, and found an effect in healthy pooled subjects, not in hypogonadal men receiving physiologic replacement doses. The review concluded that the link between TRT and sleep apnea is weak, based on methodological limitations in most studies, and that further well-designed research is needed.
Low Testosterone and Sleep Apnea Have a Circular Relationship
The relationship between sleep and testosterone levels, especially with obstructive sleep apnea, runs in both directions. Obstructive sleep apnea disrupts the deep sleep stages where most testosterone production occurs, which reduces testosterone levels and can contribute to irregular testosterone levels. Low testosterone, in turn, is associated with increased body fat, reduced upper airway muscle tone, and other factors that increase apnea risk. The Sleep Medicine Reviews comprehensive review noted that the male preponderance of sleep apnea suggests sex hormones are involved in the pathogenesis of the disorder. If you have undiagnosed sleep apnea, treating it, whether through CPAP or other methods, may significantly improve sleep and testosterone levels as a consequence of better sleep architecture, without any hormonal intervention at all.
TRT in Obese Men With Severe Sleep Apnea: What an RCT Found
A randomized placebo-controlled trial published in the European Journal of Endocrinology by Hoyos et al. studied 67 obese men with severe obstructive sleep apnea over 18 weeks. Men received either testosterone undecanoate or placebo alongside a hypocaloric diet. Testosterone treatment improved insulin sensitivity, reduced liver fat, increased muscle mass, and decreased arterial stiffness compared to placebo. The study found meaningful cardiometabolic improvements in men who would conventionally be considered contraindicated for TRT due to OSA. You may experience a different clinical conversation than you expect if both low testosterone and sleep apnea are part of your picture. The evidence no longer supports an absolute prohibition on TRT in all men with OSA, but evaluation by a licensed provider with experience in both conditions remains essential.
Natural Ways to Support Better Sleep and Testosterone at the Same Time
The most direct path to better sleep and better hormone balance is not a prescription. It is a set of lifestyle practices that benefit both systems simultaneously.
Protecting Sleep Duration and Architecture
Seven to nine hours of sleep per night is the range associated with optimal hormonal production in men, though some evidence links optimal testosterone to a sweet spot of 8 to 10 hours of sleep per night. Less than that consistently suppresses testosterone through the mechanisms described above. A consistent sleep schedule, meaning the same sleep and wake times every day including weekends, reduces the disruption to your sleep-wake cycle that irregular patterns create. A relaxing bedtime routine that lowers cortisol before sleep, along with good sleep hygiene, supports both sleep onset and the hormonal environment your body needs for nocturnal testosterone production.
Timing insight for sleep-restricted men: When sleep time is limited, staying up later and waking at a normal hour appears better for testosterone than going to bed early and waking early. A study of men restricted to 4.5 hours of sleep found that those who delayed bedtime retained higher morning testosterone than those who advanced it. This reflects that testosterone levels follow a circadian rhythm that peaks in the early morning, waking earlier can cut off that hormonal peak even when total sleep time is identical.
Resistance Training and Body Composition
Resistance training improves sleep quality through multiple pathways, including reductions in cortisol, improvements in body composition, and direct effects on sleep architecture. It also directly supports testosterone production. Reducing body fat, particularly abdominal fat, reduces the aromatase activity that converts testosterone to estrogen and lowers the adiposity-associated hormonal imbalance that disrupts both sleep and androgen levels. If you are carrying excess weight and sleeping poorly, addressing body composition through exercise and diet is one of the highest-leverage interventions for both problems simultaneously.
Treating Obstructive Sleep Apnea First
If you have loud snoring, frequent awakenings, daytime sleepiness despite adequate time in bed, or a partner who has noticed you stop breathing during sleep, evaluation for obstructive sleep apnea and other sleep disorders should happen before any testosterone assessment or treatment. Treating OSA with CPAP or another appropriate intervention can meaningfully raise testosterone levels by restoring the deep sleep stages that drive nocturnal hormone production, and broader sleep issues can also alter testosterone and mimic low-T complaints. You may find that addressing sleep apnea removes what you thought was a testosterone problem, or that it significantly improves your response to testosterone therapy if deficiency is confirmed alongside the apnea.
Managing Stress and Cortisol
Chronically elevated cortisol from psychological or physiological stress suppresses testosterone production, impairs sleep architecture, and can worsen hormone levels and broader hormonal balance. Exercise, sleep itself, reduced alcohol intake, and structured recovery time all reduce cortisol load. Alcohol in particular is worth mentioning: even moderate alcohol consumption disrupts REM sleep and suppresses testosterone, and the resulting lack of sleep can further lower it over time. If you are drinking regularly and sleeping poorly, removing or reducing alcohol is one of the most impactful single steps available to you.
If you have addressed sleep hygiene, exercise, body composition, and stress over several months and still experience persistent sleep disruption, fatigue, and low energy, a morning blood test for testosterone is a reasonable next clinical step. Your provider can evaluate whether confirmed testosterone deficiency is contributing and discuss whether treatment is appropriate based on your full clinical picture.
Frequently Asked Questions
Does low testosterone cause sleep problems?
Yes, indirectly this is how low testosterone affects sleep. Low T can disrupt sleep patterns and make it harder to fall asleep or stay asleep. Low testosterone is associated with night sweats, hormonal imbalance, and disrupted sleep architecture including reduced REM sleep and deep sleep. These effects degrade sleep quality without being the same as a primary sleep disorder.
Will testosterone therapy help me sleep better?
Not directly or reliably. A randomized controlled trial found that testosterone replacement did not improve sleep quality scores compared to placebo in men with confirmed androgen deficiency. Where TRT may help is by reducing testosterone-specific contributors to poor sleep, such as night sweats and persistent fatigue from hormonal imbalance.
Does sleep affect testosterone levels?
Yes, significantly the relationship between sleep and testosterone is closely linked, with production concentrated during sleep, particularly REM sleep. Research showing that sleep curtailment reduces circulating testosterone comes largely from studies in healthy young men. Consistently sleeping fewer than seven hours per night suppresses testosterone levels over time.
Does testosterone therapy cause sleep apnea?
The evidence that TRT causes or worsens sleep apnea is not strong. A systematic review found the caution is based on a small number of case reports with inconsistent findings, most involving supraphysiologic doses rather than standard replacement therapy. However, untreated severe sleep apnea remains a consideration before starting TRT, and your provider should screen for it.
What should I address first, poor sleep or low testosterone?
If you have symptoms or risk factors for obstructive sleep apnea, sleep evaluation comes first. Treating sleep apnea can independently improve testosterone. For men without sleep apnea, improving sleep hygiene and addressing lifestyle factors should precede any hormonal evaluation or treatment.
How many hours of sleep do I need to protect testosterone levels?
Most research supports seven to nine hours per night for optimal hormonal production in adult men. The Sleep Medicine Reviews analysis confirmed that sleep curtailment reduces circulating androgens in healthy men. Consistent deviation below seven hours is associated with measurable testosterone suppression.
Can night sweats from low testosterone be treated without TRT?
Addressing the underlying testosterone deficiency is the most direct way to resolve testosterone-related night sweats. Lifestyle interventions that support hormone balance, including weight management and stress reduction, may reduce the frequency and severity of night sweats. If confirmed low testosterone is driving them, a licensed provider can discuss appropriate treatment options.
What time of night is testosterone highest?
Testosterone production begins rising shortly after sleep onset and reaches its peak at the onset of REM sleep - typically 90 minutes into sleep in young men. The first three hours of uninterrupted sleep are the critical production window. Levels peak in the early morning hours (around 8 AM) and decline through the day. Fragmented sleep or waking too early can interrupt this peak before it fully occurs.
Does napping increase testosterone?
Short naps (20-30 minutes) can partially offset the cortisol elevation caused by poor nighttime sleep but do not replicate the full hormonal benefit of sustained overnight sleep. A nap does not produce the REM cycles or slow-wave sleep stages that drive nocturnal testosterone production. For men with sleep debt, napping is supportive but not a substitute for correcting nighttime sleep architecture.
Can melatonin help testosterone levels through better sleep?
Melatonin itself does not raise testosterone directly. However, melatonin supplementation may improve sleep onset and duration and to the extent it supports longer, higher-quality sleep, it indirectly supports nocturnal testosterone production. Melatonin has some direct antioxidant effects on testicular Leydig cells in animal studies, but this has not been established in human clinical trials.
Does alcohol affect testosterone through sleep disruption?
Yes, through two simultaneous mechanisms. Alcohol suppresses testosterone production directly and disrupts REM sleep, the stage most critical for nocturnal T production. Even moderate alcohol consumption can reduce REM sleep in the second half of the night, reducing the testosterone your body would otherwise produce during those hours. Regular evening alcohol uses compounds into measurable long-term testosterone suppression.
Can I test whether poor sleep is lowering my testosterone?
Yes. A morning blood test drawn between 7–10 AM captures testosterone at its daily peak. If your levels are borderline low and you are also sleeping poorly, retesting after two to four weeks of improved sleep quality can reveal how much of the deficit was sleep-driven versus structural. Your provider can help interpret whether a low reading reflects sleep-related suppression or confirmed androgen deficiency.
Does shift work lower testosterone?
Yes. Research links irregular sleep schedules, including night shift and rotating shift work, to lower testosterone levels. Shift work disrupts circadian rhythm, misaligns cortisol and testosterone production timing, and reduces slow-wave and REM sleep duration. Roughly one-third of American men sleep fewer than seven hours per night according to CDC data; shift workers are disproportionately represented in this group.
Conclusion
Testosterone does not improve sleep the way a sleep medication does. But the relationship between low testosterone and poor sleep is real, measurable, and bidirectional. Your sleep affects your testosterone, and poor sleep can contribute to irregular testosterone levels. Your testosterone affects your sleep. When either system breaks down, the other suffers.
If you are sleeping poorly and suspect your hormones are involved, the evidence points toward lifestyle first. Protect your sleep duration, treat sleep apnea if it is present, reduce body fat, manage stress, and cut alcohol. These steps improve both systems at once. If symptoms persist after meaningful lifestyle changes, morning blood tests are the appropriate next step because they help assess testosterone and other relevant hormone markers before treatment decisions. A licensed provider can evaluate whether confirmed testosterone deficiency is part of your picture and discuss what treatment, if any, makes sense for your specific clinical situation based on hormone testing and medically supervised, customized treatment plans rather than sleep complaints alone.
Disclaimer
This content is for educational purposes only and does not replace medical advice. Testosterone therapy and hormone-related decisions should be guided by a licensed healthcare provider.
References
- Andersen ML, Tufik S. The effects of testosterone on sleep and sleep-disordered breathing in men: its bidirectional interaction with erectile function. Sleep Med Rev. 2008;12(5):365-379. doi:10.1016/j.smrv.2007.12.003. PMID: 18519168. https://pubmed.ncbi.nlm.nih.gov/18519168/
- Luboshitzky R, Shen-Orr Z, Herer P. Middle-aged men secrete less testosterone at night than young healthy men. J Clin Endocrinol Metab. 2003;88(7):3160-3166. doi:10.1210/jc.2002-021920. PMID: 12843160. https://pubmed.ncbi.nlm.nih.gov/12843160/
- Huang G, Travison TG, Edwards RR, Basaria S. Effects of Testosterone Replacement on Pain Catastrophizing and Sleep Quality in Men with Opioid-Induced Androgen Deficiency. Pain Med. 2017;18(6):1070-1076. doi:10.1093/pm/pnw159. PMID: 27550959. https://pubmed.ncbi.nlm.nih.gov/27550959/
- Seftel AD, Kathrins M, Niederberger C. Critical Update of the 2010 Endocrine Society Clinical Practice Guidelines for Male Hypogonadism: A Systematic Analysis. Mayo Clin Proc. 2015;90(8):1104-1115. doi:10.1016/j.mayocp.2015.06.002. PMID: 26205546. https://pubmed.ncbi.nlm.nih.gov/26205546/
- Hanafy HM. Testosterone therapy and obstructive sleep apnea: is there a real connection? J Sex Med. 2007;4(5):1241-1246. doi:10.1111/j.1743-6109.2007.00553.x. PMID: 17645445. https://pubmed.ncbi.nlm.nih.gov/17645445/
- Hoyos CM, Yee BJ, Phillips CL, Machan EA, Grunstein RR, Liu PY. Body compositional and cardiometabolic effects of testosterone therapy in obese men with severe obstructive sleep apnoea: a randomised placebo-controlled trial. Eur J Endocrinol. 2012;167(4):531-541. doi:10.1530/EJE-12-0525. PMID: 22848006. https://pubmed.ncbi.nlm.nih.gov/22848006/