Yes, weed can affect testosterone, but not always how you'd expect. Some studies show lower testosterone in heavy daily users. Others found higher testosterone in occasional users. The impact depends on how much you use, how often, and your individual biology. Here's what the research actually shows.
What Is Weed and How Does It Work in Your Body?
Weed, Cannabis, THC, Marijuana: What's the Difference?
They're all the same plant.
"Weed" and "marijuana" are common names for the cannabis plant. THC (delta-9-tetrahydrocannabinol) is the chemical that causes the high.
- Cannabis sativa = the plant
- Marijuana/weed = dried flowers and leaves
- THC = main psychoactive compound
- CBD = non-psychoactive compound (doesn't get you high)
Different products contain different THC levels. Flower, edibles, concentrates, and vapes all vary in strength. More THC means stronger effects on your body and brain.
Your Body Has a Built-In System for Processing Weed
Your body has cannabinoid receptors in your brain, testes, and other tissues. These receptors are part of the endocannabinoid system, which is your body's natural regulatory network.
When you consume weed, THC binds to these receptors. This is how weed affects mood, appetite, pain...and potentially hormones.
Testicular tissue contains cannabinoid receptors, according to research published in Scientific Reports. This creates a biological pathway for weed to influence testosterone production.
How Weed Could Change Your Testosterone
Weed might lower testosterone by blocking hormone signals from your brain. But some research suggests occasional use might not have this effect or could even be associated with higher testosterone.
The mechanism works both ways depending on dose and frequency.
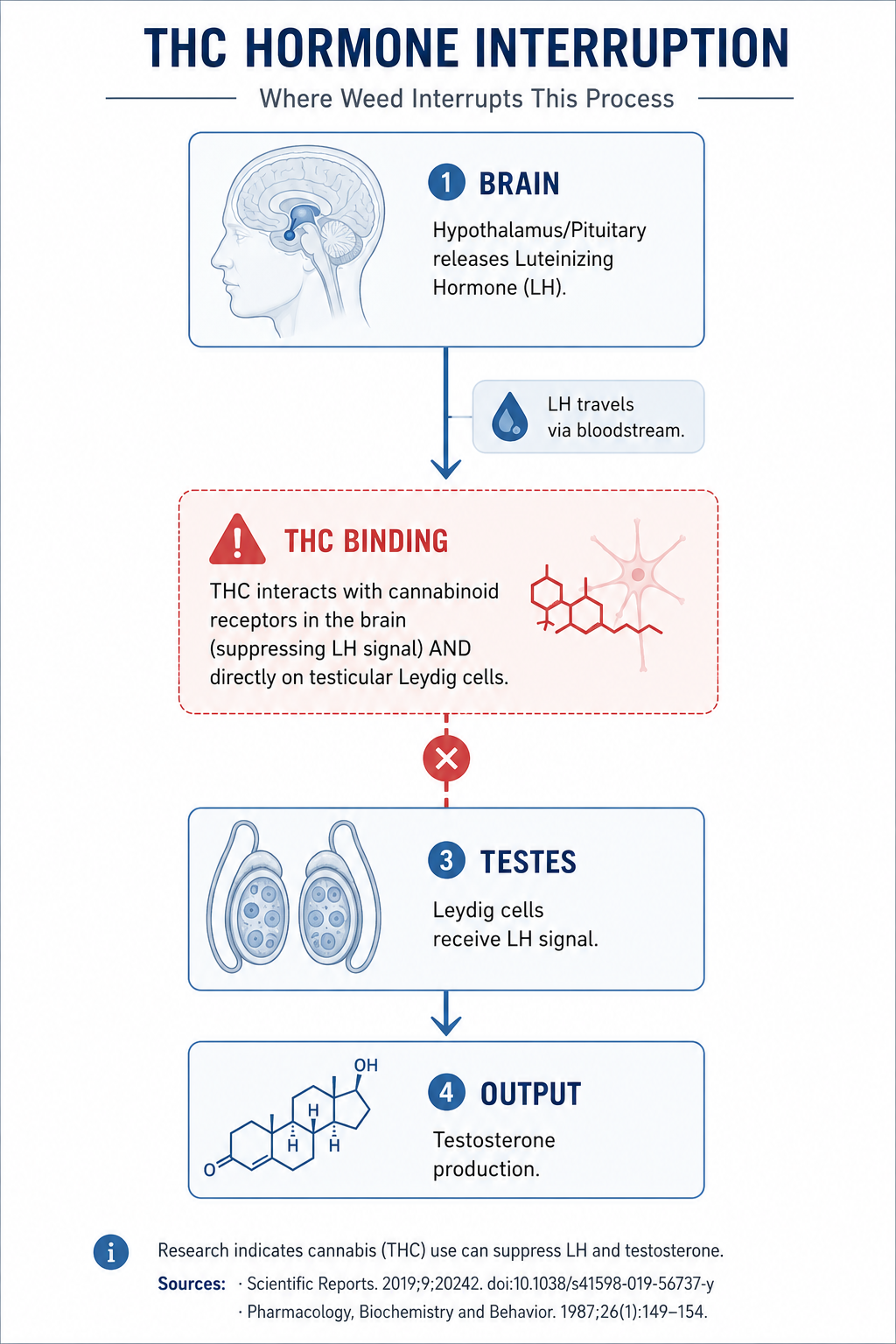
The Testosterone Production Chain
Here's how your body makes testosterone:
- Your brain releases luteinizing hormone (LH)
- LH travels through blood to your testes
- LH signals Leydig cells to produce testosterone
- Testosterone enters your bloodstream
Where Weed Interrupts This Process
Research shows THC may suppress LH release from the pituitary gland, according to a study in Pharmacology Biochemistry and Behavior. Less LH signal means less testosterone production. Higher doses suppressed LH more than lower doses.
THC may also act directly on testicular tissue. Cannabinoid receptors exist in Leydig cells which is the cells that produce testosterone. Direct THC binding could interfere with testosterone synthesis, according to research in Scientific Reports.
The Cortisol Connection
A secondary mechanism worth noting: THC can acutely elevate cortisol levels in some users.
Cortisol and testosterone have an inverse relationship. When cortisol rises, testosterone production tends to decrease.
This stress-hormone pathway is separate from the LH mechanism and may help explain why some individuals experience hormonal effects differently than others
What Research Shows About Weed and Testosterone
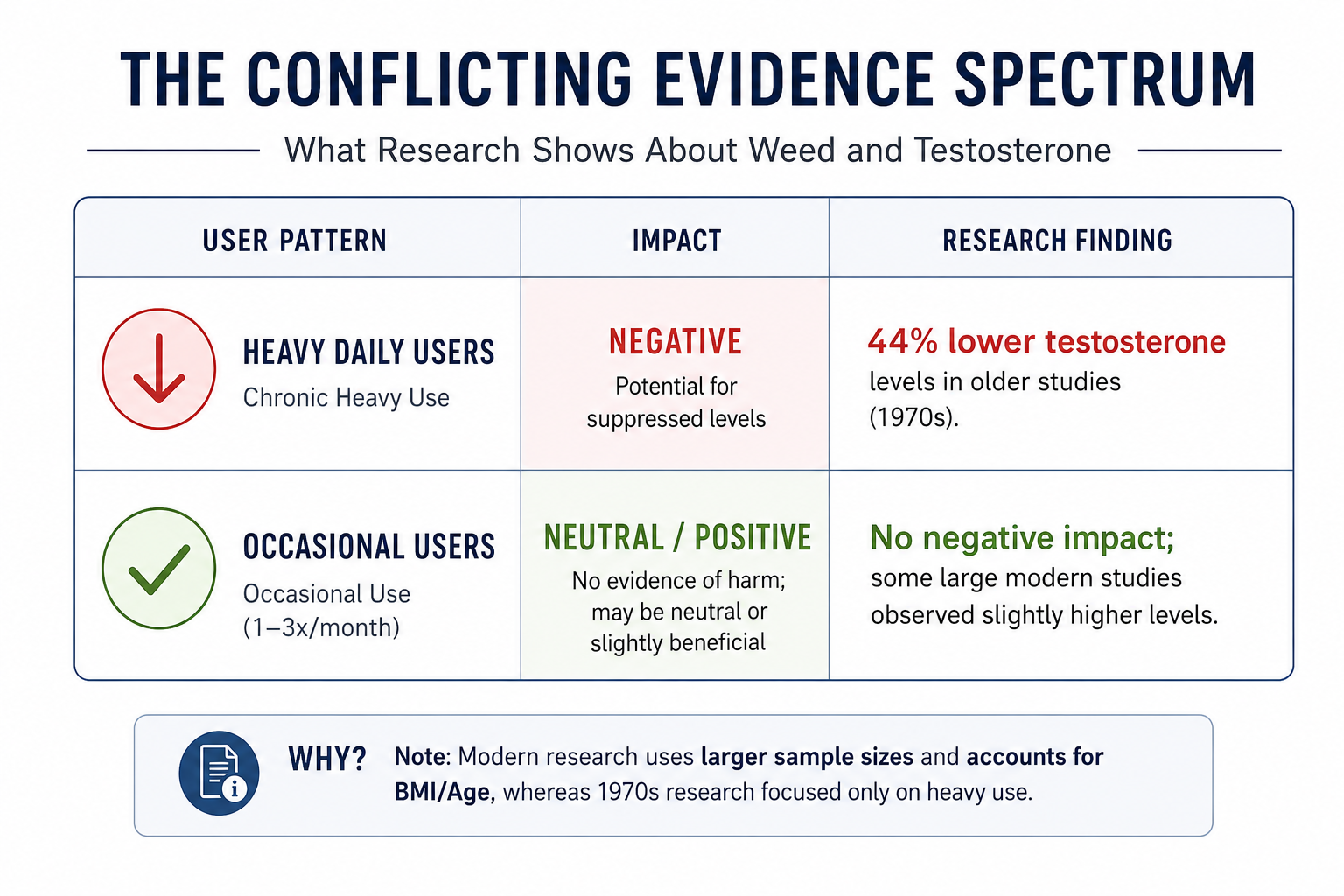
Researchers have studied marijuana consumption and male reproductive health for decades. Results conflict. Some found negative effects. Others found positive effects or no change. Here's what each body of research discovered.
Low Testosterone Levels and Reduced Sperm Quality: Reproductive health
Research from the 1970s focused on chronic heavy marijuana consumption and reproductive health.
What happened: Men who smoked heavily every day for months showed testosterone levels 44% lower than non-users. Heavy users averaged 416 ng/dL. Non-users averaged 742 ng/dL, according to findings published in the New England Journal of Medicine.
Sperm quality also declined. The same research group found reduced sperm count and sperm motility in chronic users, reported in a 1978 study.
Why it happened: Researchers believe THC suppresses luteinizing hormone (LH) from the brain. Less LH means less signal to produce testosterone. The hormone plays a critical role in testicular function.
Weak points: Small sample sizes (20-50 men). Only heavy daily users studied. No control for diet, exercise, or other substance use. Self-reported marijuana consumption with no THC content verification.
If trying to conceive, reducing cannabis use for about 3 months beforehand may be a reasonable precaution, since sperm take approximately 74 days to mature. This aligns with findings from additional reviews published in 2015 and 2019, which similarly reported associations between cannabis use and impaired semen quality, particularly sperm motility, morphology, and overall parameters.
How Low Testosterone Affects Sexual Function and Performance
Doctors became concerned about more than just hormone levels. Low testosterone affects sexual performance, energy, and muscle mass.
Animal studies showed more dramatic effects. Research on mice found high THC doses reduced testosterone and caused testicular changes, published in Science.
Why animal research matters less: Rats metabolize THC differently than humans. Doses used were 10-50 times higher than typical human consumption. Testicular changes in animals haven't been replicated consistently in people.
Effects reversed when THC stopped, a finding worth noting. Testosterone recovered within weeks in animal models. This suggests temporary impact, not permanent damage.
The Positive Effect: Higher Testosterone in Occasional Cannabis Use
More recent research found surprising results. Occasional marijuana use was associated with higher testosterone, not lower.
What happened: Men who used marijuana 1-3 times per month had the highest testosterone levels. They averaged 433 ng/dL compared to 413 ng/dL in non-users. Even frequent users (25-30 times per month) had similar levels to non-users but not lower. This finding came from a large study of 1,577 men published in Andrology.
A separate study of 1,215 young men in Denmark found no negative association between cannabis use and testosterone levels, reported in the American Journal of Epidemiology.
Why this differs from 1970s findings:
Larger sample sizes (1,500+ people versus 20-50). Controlled for age, BMI, and health conditions. Included all use patterns, not just heavy daily users. Modern research methods with objective hormone measurements.
The positive effect explained:
Occasional doses may not reach the threshold to suppress hormones. Regular users may develop tolerance to THC's hormone effects. Lifestyle factors like younger age, higher activity levels may explain higher testosterone in occasional users. Timing matters: acute effects right after use differ from baseline levels days later.
Why THC Use Shows Conflicting Results
Researchers from the University of Utah and other institutions reviewed all available evidence in a 2019 systematic review.
Conclusion: "Evidence is inconsistent."
Why studies conflict:
Sample size: 20 people produce less reliable data than 1,500 people.
Who was studied: Heavy daily users only versus mixed populations (occasional, moderate, heavy).
THC potency has changed: Weed in the 1970s contained roughly 3% THC. Modern cannabis has 15-25% THC.
Study methods: Some controlled for confounding factors. Others didn't.
Measurement timing: Some measured during active use. Others measured days or weeks after last use.
A 2018 review in European Urology Focus summarized: "Older studies of chronic heavy users suggested harm. Newer population studies found no effect or slight increase. Dose, frequency, and individual response likely determine impact."
What Actually Matters: Why Some People Are Affected and Others Aren't
The research shows one clear point: marijuana affects testosterone differently based on dose, frequency, and the person using it.
Dose and Frequency: The Pattern
Occasional use (1-3 times per month):
Evidence suggests no harm and possibly higher testosterone at this frequency based on the 2017 study. Low doses may not suppress the hormone that signals testosterone production.
Heavy daily use (4-7 times per week for months):
1970s research found lower levels in this group. Modern large-scale research found similar levels to non-users. Evidence conflicts even for heavy use.
Individual Variation: Why Results Differ Person to Person
Not everyone responds the same way to THC use.
Genetic differences: Some people have more sensitive cannabinoid receptors. The hormone system responds differently based on genetics.
Age matters: Younger men may have more resilient testosterone production. Older men may be more susceptible to disruption.
Baseline testosterone: Men with naturally high levels may tolerate more interference without clinical symptoms.
Lifestyle factors: Diet, exercise, sleep, and stress affect testosterone independent of marijuana consumption.
Tolerance: Regular users develop tolerance to many THC effects. Hormone suppression may diminish with regular use.
Reversibility: What Happens When You Stop
Animal research shows hormonal effects reverse when THC stops. A 1983 study on female primates showed tolerance developed to THC's disruptive effects on reproductive hormones. Effects were reversible.
No human studies have directly measured recovery timelines. If the mechanism involves hormone suppression from the brain, recovery should occur relatively quickly. Weeks, not months. Individual recovery time varies.
Common Claims vs What Research Actually Shows
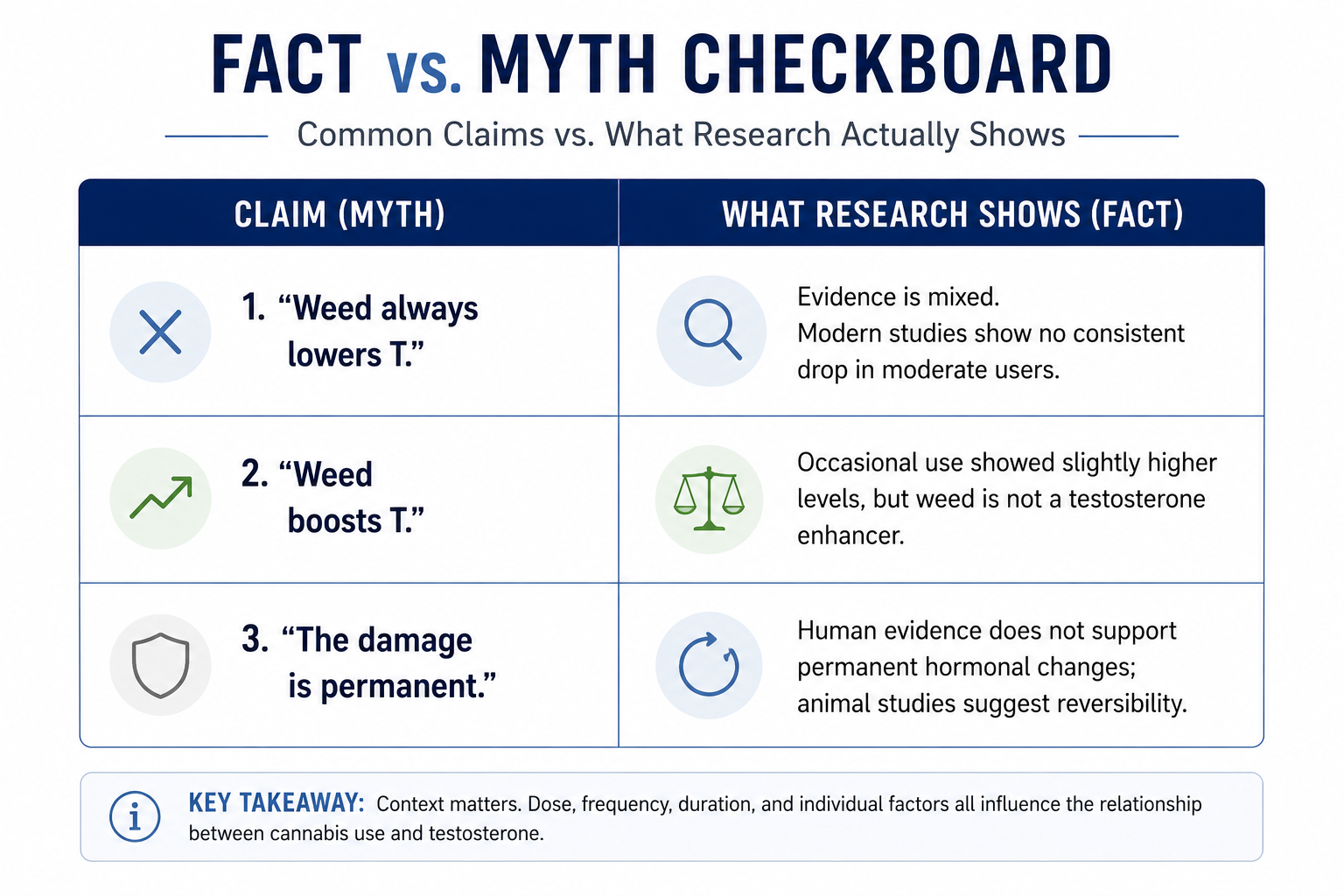
Some common claims about weed and testosterone do not fully align with current evidence. Here’s what research suggests.
Claim: “Weed always lowers testosterone.”
What research shows: Findings are mixed. Larger modern studies have not consistently shown lower testosterone levels in moderate users, and some observed slightly higher levels in occasional users.
Claim: “Weed boosts testosterone.”
What research shows: One large study reported marginally higher testosterone levels among occasional users, but the difference was small and may have been influenced by other factors. This does not support cannabis as a testosterone enhancer.
Claim: “The hormonal effects are permanent.”
What research shows: Current evidence does not support permanent hormonal changes in humans. Some animal studies suggest certain effects may reverse after exposure stops, but human data remain limited.
Claim: “CBD does not affect hormones.”
What research shows: CBD appears to behave differently from THC in available research, with less evidence of the hormonal suppression mechanisms linked to THC. However, direct human research on CBD and testosterone remains limited.
If You Use Weed and Have Low Testosterone Symptoms
Get tested. Weed use doesn't determine whether you have low testosterone. Only blood tests can confirm that.
Symptoms of Low Testosterone
- Persistent fatigue not improved by rest
- Low libido or erectile dysfunction
- Loss of muscle mass, increased body fat (especially around midsection)
- Mood changes (irritability, depression, lack of motivation)
- Brain fog, difficulty concentrating
- Reduced physical performance or endurance
When to Get Your Testosterone Tested
Testing is appropriate when:
- You have multiple symptoms affecting your quality of life
- Symptoms have been present for weeks or months, not just days
- Other causes have been ruled out (sleep disorders, thyroid issues, vitamin deficiencies)
What testing involves:
Two separate morning blood tests before 10 AM. Total testosterone measurement is standard. Free testosterone (bioavailable form) may also be measured. LH and FSH (pituitary hormones) may be checked.
If Your Testosterone Is Confirmed Low
Testosterone therapy is a medical treatment for clinically diagnosed hypogonadism.
Treatment decisions are based on:
- Confirmed low testosterone on repeated tests
- Symptoms that affect quality of life or health
- Medical evaluation ruling out other causes
- Assessment of risks and benefits by licensed provider
A doctor can advise whether cannabis use affects treatment eligibility based on your individual clinical picture.
Always disclose substance use to your healthcare provider so they can consider it when evaluating your overall health and any treatment decisions.
Practical Steps: What to Do While Waiting for Answers
Getting test results takes time. Here's what you can do:
Track your symptoms. Note energy levels, libido, mood, and physical changes over several weeks. This gives your doctor more information.
Consider your use pattern. Compare your frequency to what research studied. Occasional use shows minimal concern in recent evidence.
Plan your next steps. If testosterone comes back low, discuss treatment options. If it's normal, explore other causes for symptoms (sleep disorders, thyroid issues, vitamin deficiencies).
Don't wait if symptoms are severe. ED, extreme fatigue, or significant mood changes warrant prompt medical attention regardless of marijuana use.
FAQS
Does smoking weed every day lower testosterone?
Daily use specifically: The 1974 NEJM study studied men who smoked at least 4 times per week for a minimum of 6 months. Those subjects showed 44% lower testosterone. More recent research on daily or near-daily users (25-30 times per month) found levels similar to non-users, not dramatically lower. The pattern isn't consistent but the risk of hormonal interference increases with daily use compared to occasional use, based on available evidence.
Does smoking weed permanently lower testosterone?
No. Animal research suggests effects reverse when use stops. A 1983 study on female primates showed THC's hormonal effects were reversible. No human studies have measured permanent changes.
How much weed or marijuana use would lower my testosterone?
Studies showing reduction involved chronic heavy use, daily smoking for months or years. The 1974 research studied men who smoked at least 4 times per week for a minimum 6 months. Occasional use has not been linked to low testosterone levels in recent research.
Can CBD affect testosterone differently than THC?
More research is needed on CBD specifically. Most studies examined THC because it interacts with receptors involved in hormone regulation. CBD doesn't suppress LH the same way THC does.
If I stop, how long until testosterone recovers?
No human studies measured this directly. Animal studies showed recovery within weeks. Individual timelines likely vary based on duration and frequency of use. Testing 4-6 weeks after stopping provides individual data.
Does edible weed affect testosterone like smoking?
Delivery method hasn't been studied separately. THC is THC regardless of consumption method, though absorption differs. Effects likely depend more on dose and frequency than method.
Conclusion
Yes, weed can affect testosterone, but impact depends on dose, frequency, and the person.
Research conflicts. Heavy daily marijuana consumption in 1970s studies linked to lower testosterone and reduced reproductive health. Recent large studies found occasional users had higher levels than non-users. Even frequent users didn't show the drops researchers expected.
The biological mechanism exists for THC to suppress hormone production. But clinical impact varies widely. Occasional cannabis use shows minimal concern in modern research. Heavy daily use shows conflicting results across different studies.
If you have symptoms of low testosterone, testing is appropriate regardless of marijuana use. Talk to your doctor about getting assessed. Animal research suggests any effects reverse when use stops. Cannabis consumption does not prevent medical evaluation or approved treatment if testosterone is clinically low.
Disclaimer
This content is for educational purposes only and does not replace medical advice. Testosterone therapy and hormone-related health decisions should be guided by a licensed healthcare provider.
References
- Kolodny RC, Masters WH, Kolodner RM, Toro G. Depression of plasma testosterone levels after chronic intensive marihuana use. N Engl J Med. 1974;290(16):872-874. doi:10.1056/NEJM197404182901602. PMID: 4816961. https://pubmed.ncbi.nlm.nih.gov/4816961/
- Hembree WC, Nahas GG, Zeidenberg P, Huang HF. Changes in human spermatozoa associated with high dose marihuana smoking. Adv Biosci. 1978;22-23:429-439. PMID: 574469. https://pubmed.ncbi.nlm.nih.gov/574469/
- Nielsen JE, Rolland AD, Rajpert-De Meyts E, et al. Characterisation and localisation of the endocannabinoid system components in the adult human testis. Sci Rep. 2019;9(1):12866. doi:10.1038/s41598-019-49177-y. PMID: 31537814. https://pubmed.ncbi.nlm.nih.gov/31537814/
- Dalterio S, Bartke A. Perinatal exposure to cannabinoids alters male reproductive function in mice. Science. 1979;205(4413):1420-1422. doi:10.1126/science.451630. PMID: 451630. https://pubmed.ncbi.nlm.nih.gov/472762/
- Cone EJ, Johnson RE, Moore JD, Roache JD. Acute effects of smoking marijuana on hormones, subjective effects and performance in male human subjects. Pharmacol Biochem Behav. 1986;24(6):1749-1754. doi:10.1016/0091-3057(86)90515-0. PMID: 3005886. https://pmc.ncbi.nlm.nih.gov/articles/PMC8283823/
- Smith CG, Almirez RG, Berenberg J, Asch RH. Tolerance develops to the disruptive effects of delta 9-tetrahydrocannabinol on primate menstrual cycle. Science. 1983;219(4591):1453-1455. doi:10.1126/science.6298938. PMID: 6298938. https://pubmed.ncbi.nlm.nih.gov/6298938/
- du Plessis SS, Agarwal A, Syriac A. Marijuana, phytocannabinoids, the endocannabinoid system, and male fertility. J Assist Reprod Genet. 2015;32(11):1575-1588. doi:10.1007/s10815-015-0553-8. PMID: 26277482. https://pubmed.ncbi.nlm.nih.gov/26277482/
- Payne KS, Mazur DJ, Hotaling JM, Pastuszak AW. Cannabis and Male Fertility: A Systematic Review. J Urol. 2019;202(4):674-681. doi:10.1097/JU.0000000000000248. PMID: 30916627. https://pubmed.ncbi.nlm.nih.gov/30916627/
- Thistle JE, Graubard BI, Braunstein LZ, et al. Marijuana use and serum testosterone concentrations among U.S. males. Andrology. 2017;5(4):732-738. doi:10.1111/andr.12358. PMID: 28395129. https://pubmed.ncbi.nlm.nih.gov/28395129/
- Gundersen TD, Jørgensen N, Andersson AM, et al. Association Between Use of Marijuana and Male Reproductive Hormones and Semen Quality: A Study Among 1,215 Healthy Young Men. Am J Epidemiol. 2015;182(6):473-481. doi:10.1093/aje/kwv135. PMID: 26283084. https://pubmed.ncbi.nlm.nih.gov/26283084/
- Hsiao P, Clavijo RI. Adverse Effects of Cannabis on Male Reproduction. Eur Urol Focus. 2018;4(3):324-328. doi:10.1016/j.euf.2018.08.006. PMID: 30177436. https://pubmed.ncbi.nlm.nih.gov/30146239/