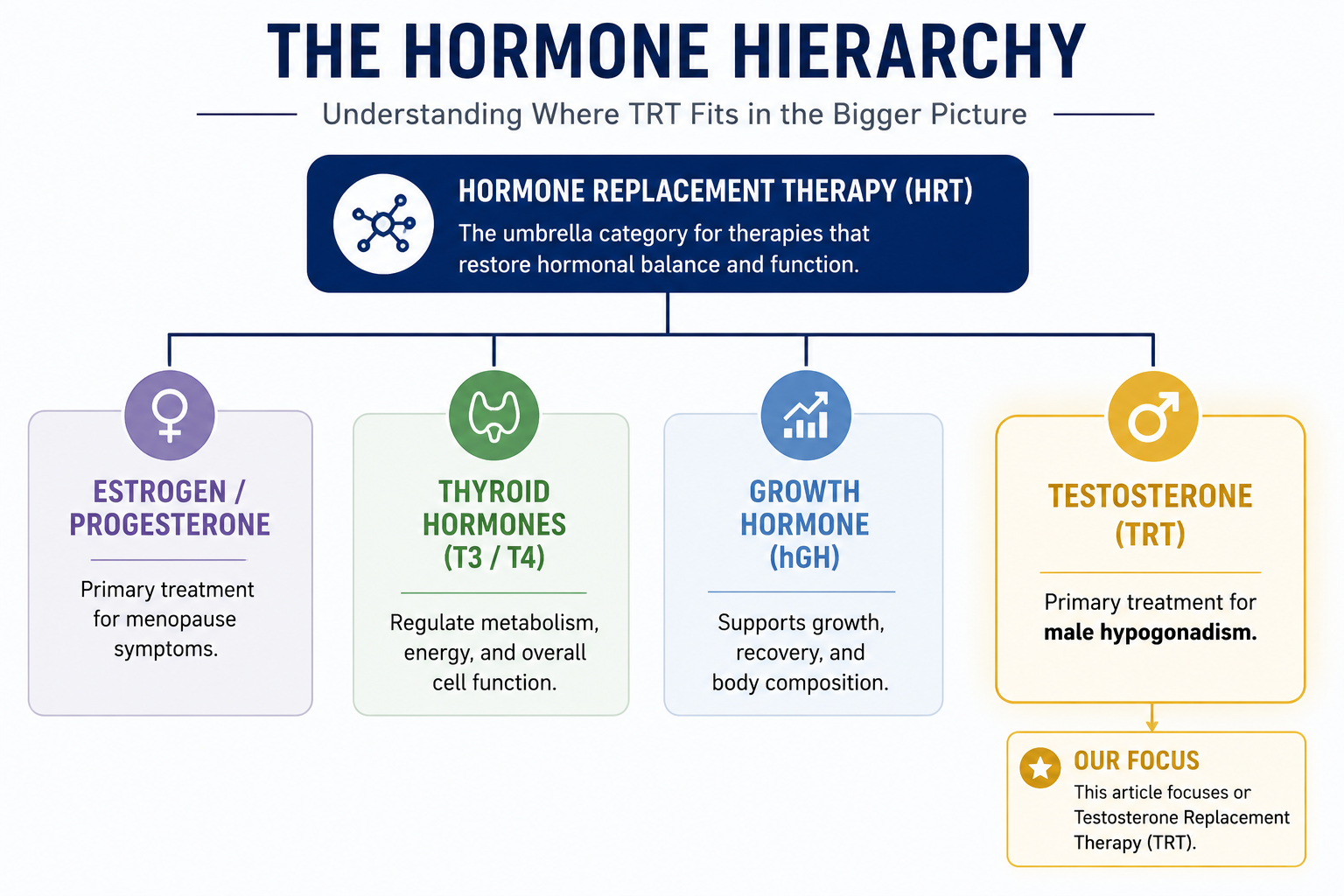
TRT (Testosterone Replacement Therapy) is a specific type of HRT (Hormone Replacement Therapy). TRT focuses exclusively on restoring testosterone levels in men with confirmed testosterone deficiency. HRT is the broader umbrella covering multiple hormones, including thyroid, growth hormone, DHEA, and testosterone. For most men presenting with hormonal symptoms, TRT is the appropriate starting point if testosterone is the only deficient hormone. Broader HRT applies when testing reveals multiple hormone deficiencies.
Disclaimer This article is for educational purposes only. It is not medical advice. It does not diagnose or treat any condition. Always consult a licensed healthcare provider before starting or changing treatment.
What is HRT?
Hormone Replacement Therapy (HRT) is a treatment approach focused on replacing hormones the body no longer produces in adequate amounts. It can involve estrogen, progesterone, testosterone, thyroid hormones, or other hormones depending on what testing confirms is deficient.
HRT is an umbrella term used for both men and women, though the hormones being treated differ. In women, it is most commonly associated with managing menopause symptoms such as hot flashes, night sweats, and mood changes. In men, hormone therapy may address testosterone or other hormonal deficiencies affecting hormonal health.
Treatment options may include bioidentical hormones or conventional synthetic formulations, depending on the clinical situation and treatment goals. While some people associate HRT with hormone optimization, proper diagnosis matters first. Symptoms like fatigue, low libido, or mood changes do not always mean a hormone deficiency.
What is TRT?
Testosterone Replacement Therapy (TRT) is a medical treatment that restores testosterone levels in men diagnosed with hypogonadism. The FDA approves TRT specifically for men with confirmed low testosterone caused by problems with the testicles, pituitary gland, or hypothalamus, not for age-related decline alone.
TRT requires a diagnosis: repeated low T blood tests plus symptoms like fatigue, decreased libido, reduced muscle mass, or mood changes. Age-related decline alone doesn't qualify.
Some people informally refer to age-related hormone changes called andropause or “male menopause,” but these are not formal medical diagnoses. Unlike menopause, testosterone decline in men tends to happen gradually over time.
TRT vs HRT: Quick Comparison
| Aspect | HRT | TRT |
| Focus | Multiple hormones | Testosterone only |
| Typical Use | Multiple hormone deficiencies | Low testosterone levels alone |
| Hormones Treated | Testosterone + Thyroid + Growth Hormone + others | Testosterone |
| Diagnosis | Multiple low hormone levels on blood tests | Low testosterone on repeated tests |
| Symptoms Addressed | Fatigue, brain fog, mood, metabolism, sexual function or sex drive, muscle loss | Fatigue, low libido, muscle loss, mood changes, erectile dysfunction |
| Research Support | Growing evidence, less extensive than TRT | Strongest evidence base |
| Monitoring Complexity | More complex (multiple hormones) | Simpler (testosterone tracking) |
| When to Consider | Blood work shows 2+ hormone deficiencies | Blood work shows low testosterone only |
Hormone Therapy Types: Understanding What Falls Under the HRT Umbrella
HRT covers several hormone treatment types: estrogen and progesterone HRT for menopause, thyroid HRT for thyroid deficiency, growth hormone HRT for GH deficiency, combined hormone therapy for multiple deficiencies, and TRT specifically for low testosterone in men.
| HRT Type | Hormones | For Whom | Why | |
| Estrogen/Progesterone HRT | Estrogen + Progesterone | Menopausal women | Hot flashes, mood changes, bone health, and other menopausal symptoms | |
| Thyroid HRT | T3, T4 | Men or women with low thyroid | Energy, metabolism, mood | |
| Growth Hormone HRT | hGH | Men or women with GH deficiency | Muscle, bone density, body composition and weight gain concerns | |
| Combined Hormone Therapy | Testosterone + Thyroid + GH (case by case) | Men with multiple confirmed hormone deficiencies | Treats more than one diagnosed deficiency, used selectively under endocrinologist guidance | |
| TRT | Testosterone only | Men with low testosterone (sometimes informally called andropause or male menopause) | Targets testosterone deficiency only |
The Key Difference
TRT focuses exclusively on testosterone. Use it when testosterone is low and other hormones are normal.
Broader HRT addresses multiple hormonal imbalances. Use it when blood work shows deficiencies in testosterone and thyroid or testosterone and growth hormone.
Is HRT the Same as TRT for Men?
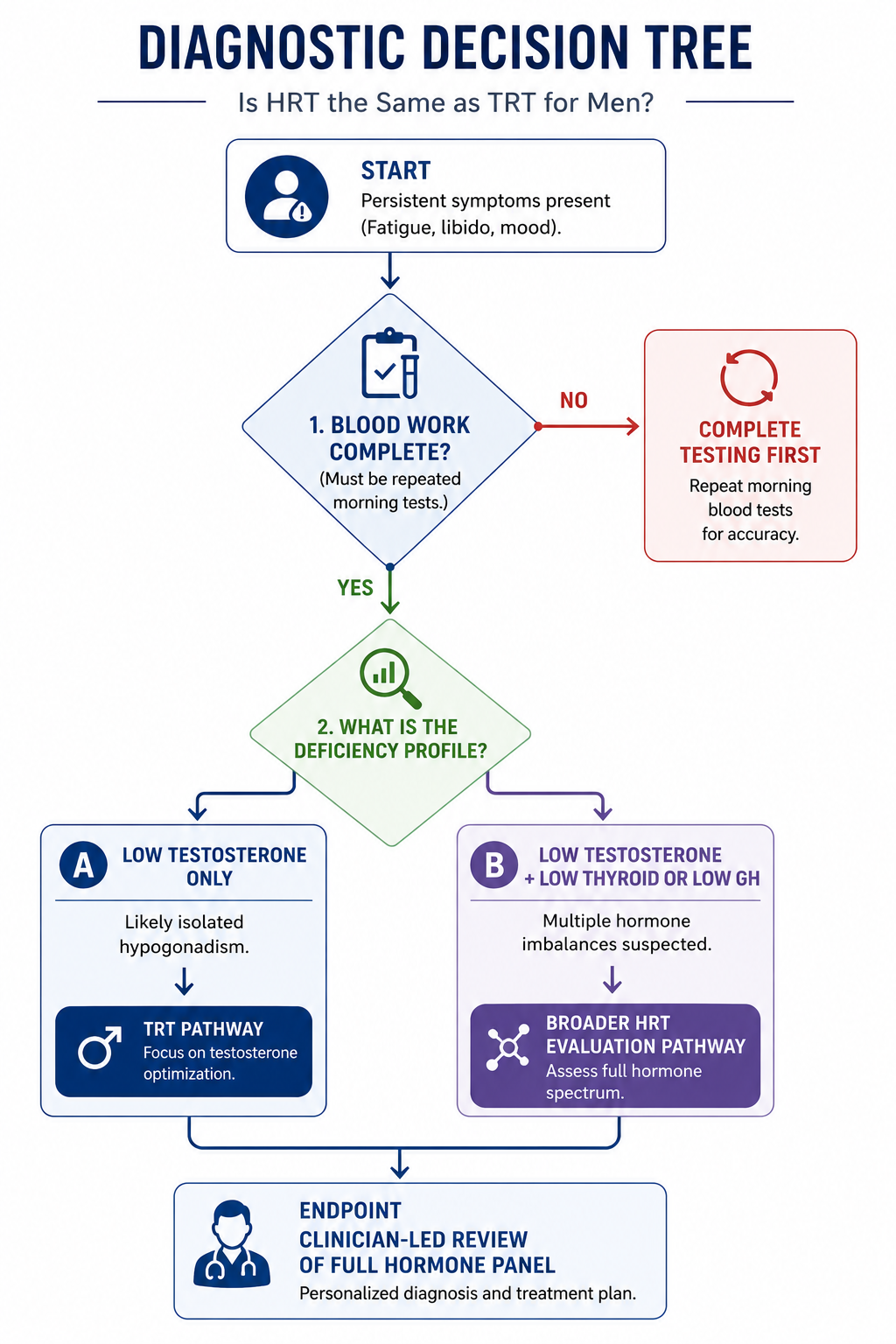
No. TRT is a type of HRT, but they're not the same. As mentioned already, HRT is the umbrella covering all hormonal treatments. TRT focuses on testosterone only. Here's how to know which one you need:
You need TRT if:
- Blood test shows low testosterone (usually <300 ng/dL)
- Your thyroid, growth hormone, and other hormones are normal
- You have symptoms: low libido, fatigue, reduced muscle mass, mood changes, erectile dysfunction
- Your doctor rules out other hormone problems
You need broader hormone replacement therapy (HRT) if:
- Blood test shows low testosterone and low thyroid (high TSH, low Free T4)
- Blood test shows low testosterone and low growth hormone (low IGF-1)
- You're on TRT with good testosterone levels, but still feel fatigued or have mood problems
- Your doctor finds multiple endocrine system problems
Cost context (2026): Injectable testosterone (cypionate/enanthate) typically costs $30 to 100/month as a generic. Testosterone gels and brand-name formulations run $150 to 400/month. Broader HRT adding thyroid, growth hormone, or DHEA therapy increases costs significantly. Verify current formulary coverage with your insurance before selecting a formulation.
What Are the Symptoms of Low Testosterone?
Common symptoms of low testosterone in men include decreased libido, erectile dysfunction, persistent fatigue, reduced muscle mass, mood changes, and increased body fat. In long-term untreated cases, bone density loss can occur. Blood testing is the only way to confirm whether low testosterone is the actual cause.
Low testosterone can affect men of any age but becomes more common as men age. Symptoms typically develop gradually rather than suddenly, which can make them easy to attribute to other causes like aging, stress, or lifestyle factors. The most common symptoms include:
Sexual function changes
- Decreased libido or sex drive
- Erectile dysfunction or fewer spontaneous erections
- Reduced morning erections
Energy and physical changes
- Persistent fatigue not relieved by sleep
- Reduced muscle mass and strength despite normal activity
- Increased body fat, especially around the abdomen
- Reduced exercise tolerance
Mood and cognitive changes
- Irritability or mood changes
- Depression or low mood
- Reduced motivation or drive
- Brain fog or reduced cognitive sharpness
Long-term physical changes
- Bone density loss (in untreated cases over time)
- Reduced body hair
- Decreased testicular size in some cases
Why a Blood Test Is Required
Symptoms alone aren't enough for a low T diagnosis. Many of these symptoms overlap with thyroid problems, depression, sleep disorders, diabetes, and other conditions. Diagnosis requires two morning testosterone tests on separate days plus a full hormone panel that includes LH, FSH, prolactin, and thyroid markers. A proper workup rules out other causes before treatment is considered.
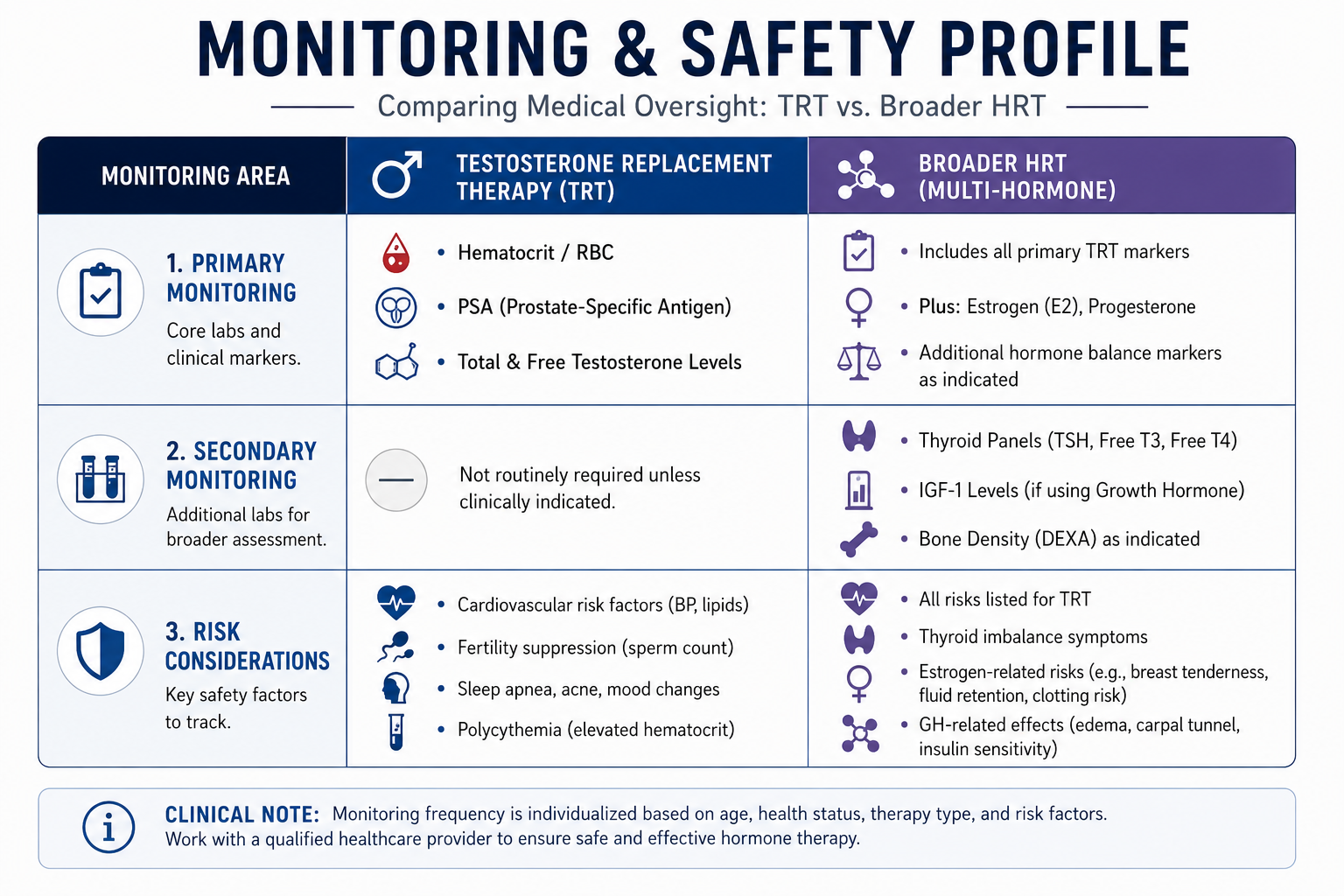
TRT Side Effects and Risks: What Research Shows
Common TRT side effects include acne, oily skin, fluid retention, and mood changes. More serious risks involve elevated red blood cell counts and reduced fertility. The 2023 TRAVERSE trial found no significant increase in major adverse cardiovascular events in properly screened men, though it did identify elevated rates of atrial fibrillation, pulmonary embolism, and acute kidney injury.
Common Side Effects
Most TRT side effects are manageable with proper monitoring and dose adjustments. These include:
- Acne or oily skin
- Fluid retention (mild swelling)
- Mood changes, especially during dose adjustment periods
- Sleep disturbances in some cases
- Skin reactions at application sites for topical methods
- Breast tissue tenderness or gynecomastia in some cases
Serious Considerations
Some risks require more careful monitoring and may affect whether TRT is appropriate:
Cardiovascular safety. The 2023 TRAVERSE trial, the largest cardiovascular safety study of TRT, found no significant increase in heart attacks or strokes among carefully screened men with hypogonadism. However, the trial did identify elevated rates of atrial fibrillation, pulmonary embolism, and acute kidney injury, meaning TRT still requires ongoing monitoring.
Polycythemia. TRT can increase red blood cell production, raising hematocrit levels. This is why hematocrit monitoring is part of standard TRT care.
Prostate concerns. TRT is not recommended for men with active prostate cancer. PSA monitoring is part of routine TRT care to catch any prostate changes early.
Fertility suppression. TRT signals the brain to stop natural testosterone and sperm production. This can lead to azoospermia (no measurable sperm) within months. Men who want to preserve fertility should discuss alternatives like clomiphene or HCG with their doctor before starting TRT.
Sleep apnea aggravation. In rare cases, TRT can worsen pre-existing sleep apnea.
Long-term research is ongoing. The TRAVERSE trial answered key cardiovascular questions, but the long-term effects of TRT over decades of use remain an active area of research. Anyone on TRT should remain in active care with regular bloodwork and clinical follow-up.
Bioidentical Hormones vs Synthetic Hormones in HRT
Bioidentical hormones are structurally identical to the hormones your body naturally produces. Synthetic or conventional hormones are chemically modified versions designed to produce similar therapeutic effects. Both can be used for replacing hormones when medically appropriate.
Key differences:
- Bioidentical hormones: Match the body’s natural hormone structure.
- Synthetic hormones: Modified compounds with similar hormone activity.
- FDA-approved bioidentical options exist: These are different from compounded hormone products.
- Compounded “bioidentical” hormones: Customized formulations often marketed for hormone optimization, but they do not undergo the same FDA approval standards as commercial products.
- Safety claims vary: “Bioidentical” does not automatically mean safer or more effective.
Some patients prefer personalized compounded options, while others use standardized FDA-approved therapies. The best choice depends on symptoms, treatment goals, medical history, and provider guidance, not marketing labels alone.
DHEA and Cortisol: Other Hormones in Men's Hormonal Health
Whether a man receives bioidentical or synthetic hormones depends partly on which hormones need replacing. Beyond testosterone, two adrenal hormones frequently surface in men's broader hormonal evaluations: DHEA and cortisol.
DHEA (dehydroepiandrosterone) is produced by the adrenal glands and converts downstream into testosterone and estrogen. Levels peak in a man's 20s and decline steadily with age. According to research published in Vitamins and Hormones, DHEA and its sulfated form can be metabolized by most tissues into active androgenic compounds. A man with low DHEA may show symptoms identical to low testosterone when the actual deficiency sits at the adrenal level, not the testes. Testing DHEA-S alongside testosterone clarifies where the problem originates.
Cortisol, also adrenal-produced, works in direct opposition to testosterone. A study in Fertility and Sterility examining overtraining in five endurance-trained men documented a strong inverse correlation between rising cortisol and falling testosterone during the overtraining period (r = -0.92), with both hormones returning to baseline after training volume was reduced.
More broadly, chronic elevation of cortisol from any cause is understood to suppress the hypothalamic-pituitary-gonadal axis - the same pathway that drives testosterone production - through direct inhibition of GnRH and LH secretion. This is the biological mechanism behind the stress-testosterone connection discussed in the next section.
When blood work confirms an adrenal component alongside low testosterone, treatment moves beyond TRT into broader HRT territory. This is why a complete hormone panel matters, not just a testosterone reading.
Can Lifestyle Changes Replace HRT or TRT?
For men with diagnosed hypogonadism, lifestyle changes alone usually can't fully replace medically necessary TRT. However, several lifestyle factors significantly affect testosterone production, and for men with borderline-low T, optimizing these factors should be tried first.
Lifestyle factors that affect testosterone production include:
Sleep quality and duration. Most testosterone production happens during deep sleep. Chronic sleep deprivation or untreated sleep apnea can significantly lower testosterone levels. Aim for 7-9 hours of quality sleep.
Body composition: Excess body fat, particularly abdominal fat, converts testosterone to estrogen through an enzyme called aromatase.
Weight loss alone can sometimes restore normal testosterone levels in men with obesity-related low T.
Resistance training: Regular strength training has been shown to support natural testosterone production. Both compound lifts and moderate-intensity weight training help.
Stress management: Chronic stress elevates cortisol, which suppresses testosterone. Stress management practices, meditation, breathwork, adequate recovery between workouts, work-life balance, support healthier hormone levels.
Diet quality: Adequate zinc, vitamin D, magnesium, and healthy fats all support testosterone production. Severe caloric restriction can lower testosterone, as can highly processed diets low in micronutrients.
Alcohol consumption: Heavy or chronic alcohol use lowers testosterone and impairs liver function involved in hormone metabolism.
When Lifestyle Changes Are Enough
For men with borderline-low testosterone and addressable lifestyle factors (poor sleep, obesity, chronic stress), 6-12 months of focused lifestyle optimization may be discussed as a first step with their provider before considering TRT. This often improves not just testosterone but overall well being.
When Lifestyle Isn't Enough
For men with confirmed hypogonadism, meaning the testicles, pituitary, or hypothalamus aren't producing or signaling testosterone properly, lifestyle changes won't fix the underlying problem. These men need medical treatment regardless of how optimized their lifestyle factors become.
The right approach is to work with a qualified provider to identify whether your low T is lifestyle-driven, medically driven, or both.
HRT for Women vs TRT for Men: Key Differences
Women's HRT and men's TRT serve different purposes, treat different hormones, and have different risk profiles. Women's HRT typically combines estrogen and progesterone to manage menopause symptoms, while TRT for men focuses on testosterone replacement for hypogonadism.
Different Purposes
Women's HRT primarily treats menopause symptoms hot flashes, night sweats, vaginal dryness, mood changes, and bone density loss that accompanies the drop in estrogen during and after menopause. Some women also use HRT to manage early menopause or surgical menopause.
Men's TRT primarily treats hypogonadism, a medical condition where the testicles, pituitary, or hypothalamus aren't producing or signaling testosterone normally. Unlike menopause, which has a clear hormonal milestone, men's testosterone decline is gradual and testing is required to confirm whether levels are truly deficient.
Different Risk Profiles
Both therapies have well-studied risks, but they're different:
Women's HRT considerations
- Breast cancer risk varies depending on the regimen. The Women's Health Initiative (WHI) study found combined conjugated equine estrogen plus medroxyprogesterone acetate (MPA) - a synthetic progestogen - was associated with increased breast cancer risk in some groups. Estrogen-only HRT in women without a uterus actually showed a reduced breast cancer risk in the WHI. These findings apply to the specific formulations tested; bioidentical progesterone may carry a different risk profile, though evidence remains under active investigation.
- Cardiovascular and stroke risk vary by age at initiation and underlying health status.
- Endometrial cancer risk requires progesterone protection if a uterus is present.
Men's TRT considerations
- Cardiovascular monitoring required (especially atrial fibrillation, per TRAVERSE 2023)
- Prostate monitoring required (PSA tracking)
- Fertility suppression, significant concern for younger men
- Polycythemia risk requires hematocrit monitoring
Why Both Need Proper Clinical Workup
Whether you're a woman considering HRT or a man considering TRT, proper hormone testing, symptom evaluation, and risk assessment matter equally. Both treatments use FDA-approved bioidentical and synthetic options, and both require ongoing monitoring throughout treatment.
The right framework for either therapy is the same: confirmed lab testing, symptom correlation, evaluation of underlying causes, and ongoing partnership with a qualified provider.
When are HRT and TRT most appropriate? At What Age is it Too Late for HRT?
No, it's not too late based on age alone. What matters is your blood work and symptoms, not your age.
Testosterone levels naturally decline after age 30, roughly 1 to 2% per year, according to large population studies. The question isn't "am I old enough" but rather "do I have confirmed low testosterone causing real symptoms?"
Research shows a 45-year-old with serious symptoms and confirmed low testosterone may benefit from TRT. A 70-year-old with normal testosterone but fatigue probably doesn't have a testosterone deficiency; the fatigue likely comes from something else.
A trial in The New England Journal of Medicine looked at men over 65 with low testosterone. TRT produced modest benefits for sexual function and bone density loss specifically, though it did not produce significant improvements in vitality, walking ability, or memory across the trial population. A man at 75 with confirmed low testosterone levels and real symptoms may benefit from TRT. A man at 45 with normal testosterone won't, regardless of age.
Bottom line: It's not too late based on age. It's too late only if your doctor finds no hormone deficiencies or if you have serious health conditions that make hormone therapy unsafe.
FAQs
Do celebrities use TRT?
Some public figures have openly discussed testosterone replacement therapy, helping normalize the conversation around men's hormonal health. However, treatment decisions are individualized and require clinical evaluation, bloodwork, and medical supervision.
Which is better, TRT or HRT?
Neither is "better"—the right choice depends on your overall hormonal health and hormonal profile. As discussed earlier, if only testosterone is low, TRT is appropriate. If multiple key hormone productions are deficient, broader HRT is needed to restore normal levels.
At what age should men start TRT or HRT?
Age alone doesn't determine this. As covered in the age section, what matters is confirmed hormonal deficiency on repeated blood tests plus symptoms. This can happen at 40 or 70.
How long should a man be on TRT or HRT?
That depends on the underlying cause. Some men require lifelong therapy. Others might adjust or stop if the underlying condition resolves. Your provider determines duration based on your specific overall well-being.
Why do doctors not recommend TRT?
Some doctors hesitate because of older studies that raised cardiovascular safety questions. The 2023 TRAVERSE trial, the largest cardiovascular safety study of TRT to date, found no significant increase in major adverse cardiovascular events in carefully screened men with hypogonadism. However, the trial did identify elevated rates of atrial fibrillation, pulmonary embolism, and acute kidney injury, meaning TRT still requires ongoing monitoring.
What Are the Different TRT Administration Methods?
TRT is available through several FDA-approved delivery methods: intramuscular or subcutaneous injections (cypionate, enanthate), daily topical gels and creams (AndroGel, Testim), transdermal patches, nasal gel (Natesto, three times daily), subdermal pellets inserted every 3 to 6 months, and oral testosterone undecanoate (Jatenzo, Kyzatrex) taken twice daily with food. Injections are the most widely used and cost-effective. For men concerned about fertility preservation, off-label alternatives such as clomiphene or enclomiphene stimulate natural testosterone production without suppressing it, discuss suitability with your provider.
Conclusion
HRT vs TRT for men is ultimately a question of scope. TRT addresses testosterone alone. HRT addresses multiple hormones. For most men seeking hormonal balance, TRT is the appropriate medical treatment, research is strongest for testosterone-specific therapy, and isolated testosterone deficiency is more common than multi-hormone dysfunction.
Broader HRT applies when confirmed lab work shows deficiencies in multiple hormone systems. Neither therapy is appropriate without confirmed lab testing and clinical evaluation.
The key is understanding which treatment matches your actual hormonal profile and that requires proper testing and professional assessment.
References
Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: An Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018 May;103(5):1715-1744. doi:10.1210/jc.2018-00229. PMID: 29562364. https://pubmed.ncbi.nlm.nih.gov/29562364/
Bhasin S, Travison TG, Pencina KM, et al. Prostate Safety Events During Testosterone Replacement Therapy in Men With Hypogonadism: A Randomized Clinical Trial. JAMA Netw Open. 2023;6(12):e2348692. doi:10.1001/jamanetworkopen.2023.48692. PMID: 38150256. https://pubmed.ncbi.nlm.nih.gov/38150256/
Snyder PJ, Bhasin S, Cunningham GR, et al. Effects of testosterone treatment in older men. N Engl J Med. 2016 Feb;374(7):611-624. doi:10.1056/NEJMoa1506119. PMID: 26886521. https://pubmed.ncbi.nlm.nih.gov/26886521/
Snyder PJ, Kopperdahl DL, Stephans-Shields AJ, et al. Effects of testosterone treatment on bone mineral density in men over 65 years of age with low testosterone. J Clin Endocrinol Metab. 2015 Jun;100(8):3170-3178. doi:10.1210/jc.2015-1872. PMID: 25898953. https://pubmed.ncbi.nlm.nih.gov/25898953/
Walther A, Breidenstein J, Miller R. Association of Testosterone Treatment With Alleviation of Depressive Symptoms in Men: A Systematic Review and Meta-analysis. JAMA Psychiatry. 2019;76(1):31–40. doi:10.1001/jamapsychiatry.2018.2734. PMID: 30694318. https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2712976
Lincoff AM, Bhasin S, Flevaris P, et al. Cardiovascular safety of testosterone-replacement therapy. N Engl J Med. 2023 Jun;389(2):107-117. doi:10.1056/NEJMoa2215025. PMID: 37326322. https://pubmed.ncbi.nlm.nih.gov/37326322/
Roberts AC, McClure RD, Weiner RI, Brooks GA. Overtraining affects male reproductive status. Fertil Steril. 1993;60(4):686-92. doi:10.1016/s0015-0282(16)56223-2. PMID: 8405526. https://pubmed.ncbi.nlm.nih.gov/8405526/
Klinge CM, Clark BJ, Prough RA. Dehydroepiandrosterone Research: Past, Current, and Future. Vitam Horm. 2018;108:1-28. doi:10.1016/bs.vh.2018.02.002. PMID: 30029723. https://pubmed.ncbi.nlm.nih.gov/30029723/