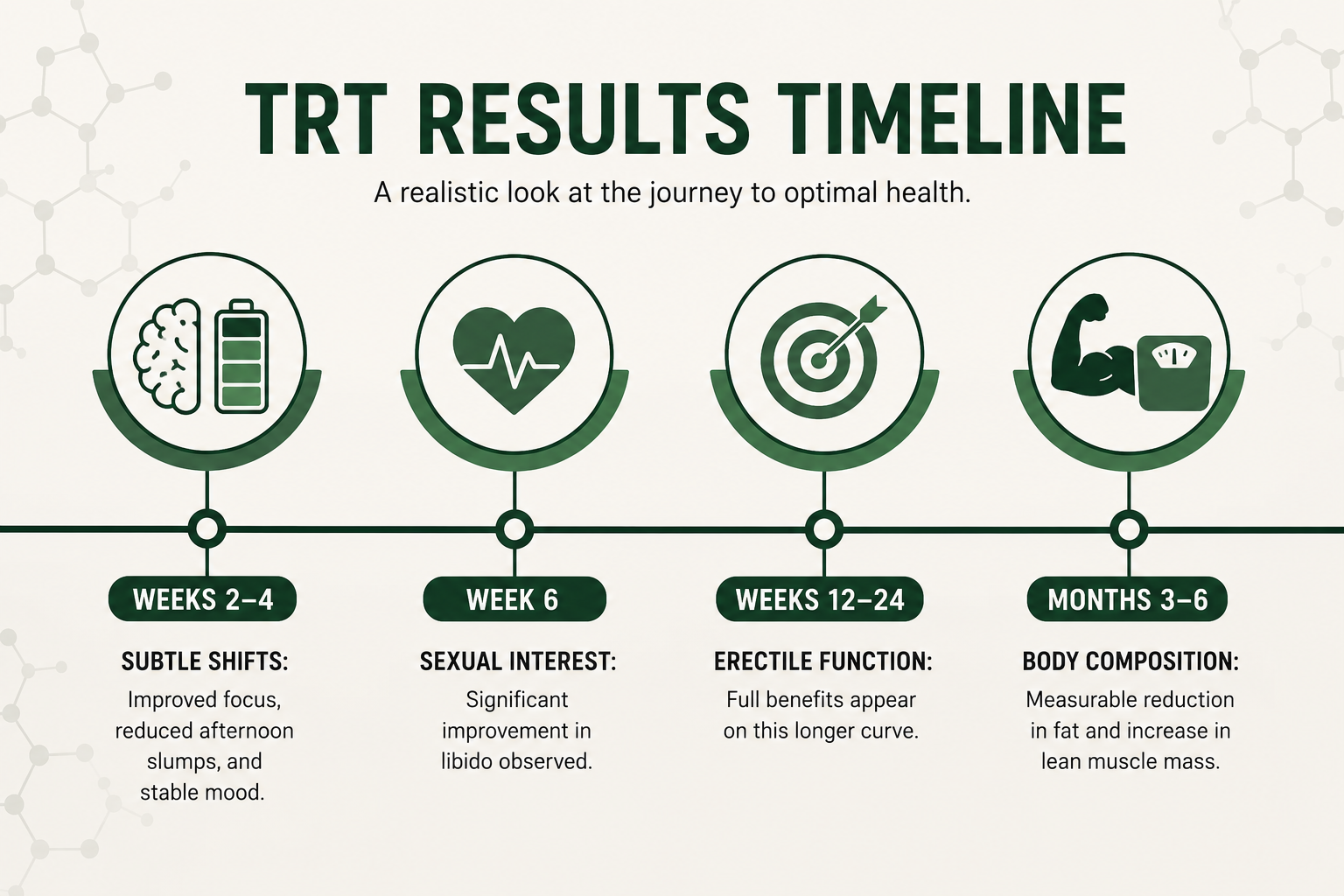
Starting testosterone replacement therapy (TRT) is a gradual process rather than an instant transformation, requiring both patience and medical oversight. While many men report subtle improvements in mood and energy levels within two to four weeks, other benefits follow a longer timeline: sexual interest typically improves by week six, while significant changes in erectile function and body composition, such as increased lean muscle and fat loss, generally take three to six months to manifest. Success with TRT depends on realistic expectations, consistent resistance training, and diligent, ongoing lab monitoring to ensure health markers like hematocrit remain within safe ranges throughout your treatment.
Starting TRT is not a switch you flip. It is a process your body responds to over weeks and months, and the timeline rarely matches what you may have read online or heard from someone at the gym.
Low testosterone in men with confirmed male hypogonadism is a treatable medical condition, and testosterone replacement therapy TRT is the primary clinical option for restoring hormone levels to the normal range. When it works well, the effects can be life changing. When expectations are misaligned, men either stop therapy too early because they expected results that take months to appear, or they miss early warning signs because nobody told them what to monitor.
This article gives you an honest, research-backed picture of what starting TRT actually looks like, what subtle changes come first, what takes longer, and what risks require your attention from the very beginning.
Starting TRT: What to Expect in the First Few Weeks
The first few weeks after starting TRT are about stabilisation, not transformation. Your body is adjusting to exogenous testosterone for the first time, your baseline labs are being compared against early results, and your hormone levels are moving toward a new baseline.
The Changes You May Notice First
Mood and energy often shift before anything physical does, and many patients notice these early changes as subtle shifts rather than dramatic effects. Many men begin to notice fewer afternoon slumps, a quieter mental noise, and a slightly sharper sense of drive and sharper focus within two to four weeks. These are not dramatic changes. They are subtle, and you may not register them consciously until you look back.
Sexual interest is typically one of the earlier signals, with sex drive often starting to improve in the same early window. A randomised controlled trial published in Andrology studying 199 hypogonadal men with type 2 diabetes found that sexual desire improved significantly within 6 weeks of starting testosterone undecanoate , and that this early improvement in sexual interest predicted later improvements in erectile function at 30 weeks. This is a clinically useful pattern. If you are not noticing any shift in low libido by week six, that is worth discussing with your healthcare provider.
Morning erections may begin to return during this early window, though their return is not universal and depends heavily on psychological factors, sleep quality, and how long your testosterone levels have been suppressed.
What Is Actually Happening in Your Body
Your body is adjusting to the introduction of exogenous testosterone, which suppresses the hypothalamic signal to produce testosterone naturally. Hormone levels are in flux. Your healthcare provider will typically schedule early blood tests to confirm your total testosterone is tracking toward the normal range and to catch any early changes in red blood cell count, estrogen levels, or other markers.
Do not adjust your dose based on how you feel in week one or two. That is not enough time for your body to reach stable hormone levels, and premature dose changes are one of the most common reasons TRT patients experience erratic results.
Weeks 3 to 6: The Window Where Subtle Changes Begin to Stack
By weeks three to six, your testosterone levels are approaching a more stable state, particularly with weekly injections or daily testosterone gel application. This is where many men begin to notice changes they can actually name.
Energy Levels and Brain Fog
Low energy and brain fog are two of the symptoms men with low testosterone report most consistently before starting treatment. A clinical review in Nature Reviews Urology confirmed that symptomatic benefits of testosterone therapy may not manifest for several weeks to many months, with energy typically appearing earlier than physical changes. You may find you are getting more done in the morning, that your thinking feels cleaner, and that the mental clarity you had lost gradually starts returning as brain fog lifts into cognitive clarity. These are real but quiet shifts. They are not the same as feeling medicated or artificially energised. They feel more like returning to baseline.
Mood Changes and Reduced Irritability
Testosterone plays a direct role in emotional regulation. As your hormone levels stabilise in the therapeutic range, irritability, emotional flatness, and low-grade depressive feelings may ease, though mood can still be shaped by other factors such as sleep, stress, and daily habits. This use has not been approved by the FDA as a treatment for depression or mood disorders, but mood changes linked to testosterone deficiency can respond to hormone restoration. You may notice you are less reactive, more patient, and more present in daily life. The people around you may notice before you do.
Months 2 to 3: Noticeable Improvements in Sexual Function
Sexual function improvements deepen during months two and three as your hormone levels remain consistently elevated. This is where the gap between sexual interest returning and full erectile function returning often becomes clear.
Erectile Function Takes Longer Than Libido
This distinction matters. Sexual interest tends to improve earlier. Erectile function follows on a longer curve. A clinical study in the Journal of Sexual Medicine followed 22 hypogonadal men on long-acting testosterone undecanoate and found that while testosterone levels normalised within 6 to 8 weeks, in 9 of 12 men who showed erectile function improvement, that improvement only became apparent after 12 to 24 weeks of treatment. If your sexual interest has returned but your erectile function has not yet followed, you are likely still within the normal response window. Give it time before concluding TRT is not working.
Physical Performance Begins to Shift
Physical performance and physical activity tolerance are also beginning to change by months two and three, particularly if you are resistance training consistently. A large randomised controlled trial in the Journal of Clinical Endocrinology and Metabolism following 227 hypogonadal men on transdermal testosterone gel found that muscle strength in the leg press increased by 11 to 13 kg across all treatment groups by 90 days. You will not look dramatically different yet, but if you are training consistently, you may find that your recovery is better, your sessions feel more productive, and you are responding to resistance training in ways that you were not before.
Months 3 to 6: Body Composition Changes Become Visible
This is where the body composition changes that many men expect from the beginning start to become visible. Lean muscle mass increases. Reduced fat, particularly visceral fat, becomes measurable. Water retention that may have appeared in early weeks begins to normalise as your hormone levels stabilise.
What the Research Shows on Fat and Muscle
A randomised controlled trial published in BMC Medicine studied 100 obese hypogonadal men on testosterone undecanoate versus placebo over 56 weeks. By the end of the study, the testosterone-treated group had significantly greater reductions in fat mass and visceral fat compared to placebo, and while both groups lost lean mass during the caloric restriction phase, testosterone-treated men regained lean muscle mass during the weight maintenance phase, contrasting directly with the placebo group who did not. This is a meaningful finding for you: TRT supports the preservation and regrowth of lean muscle mass in ways that diet and physical activity alone do not produce when testosterone levels are deficient.
Realistic Expectations About Body Composition
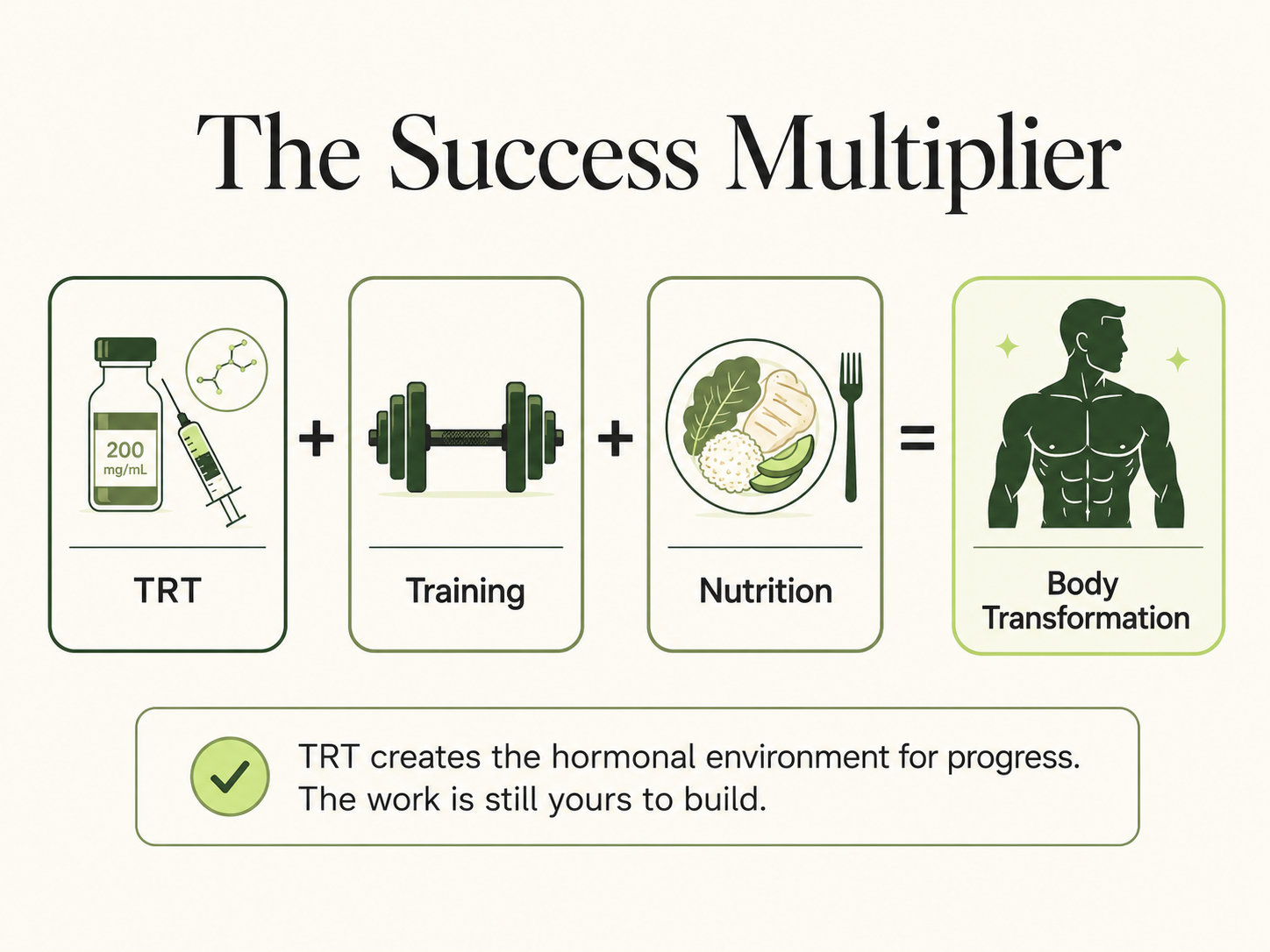
Body composition changes on TRT are real but not rapid. TRT alone has not conclusively been shown to improve overall quality of life, even when body composition improves. You will not look like a different person at three months. If you are also eating a balanced diet, managing sleep quality, and training consistently, the changes compound meaningfully over six months to a year. TRT creates a hormonal environment in which your body can respond properly to the work you are doing. It does not do the work for you.
All the Difference Is in the Details: Fine Tuning Your Protocol
TRT is not a set-and-forget treatment. Fine tuning is an ongoing part of the process, and it is where most of the long-term outcomes are actually determined.
Why Lab Monitoring Is Non-Negotiable
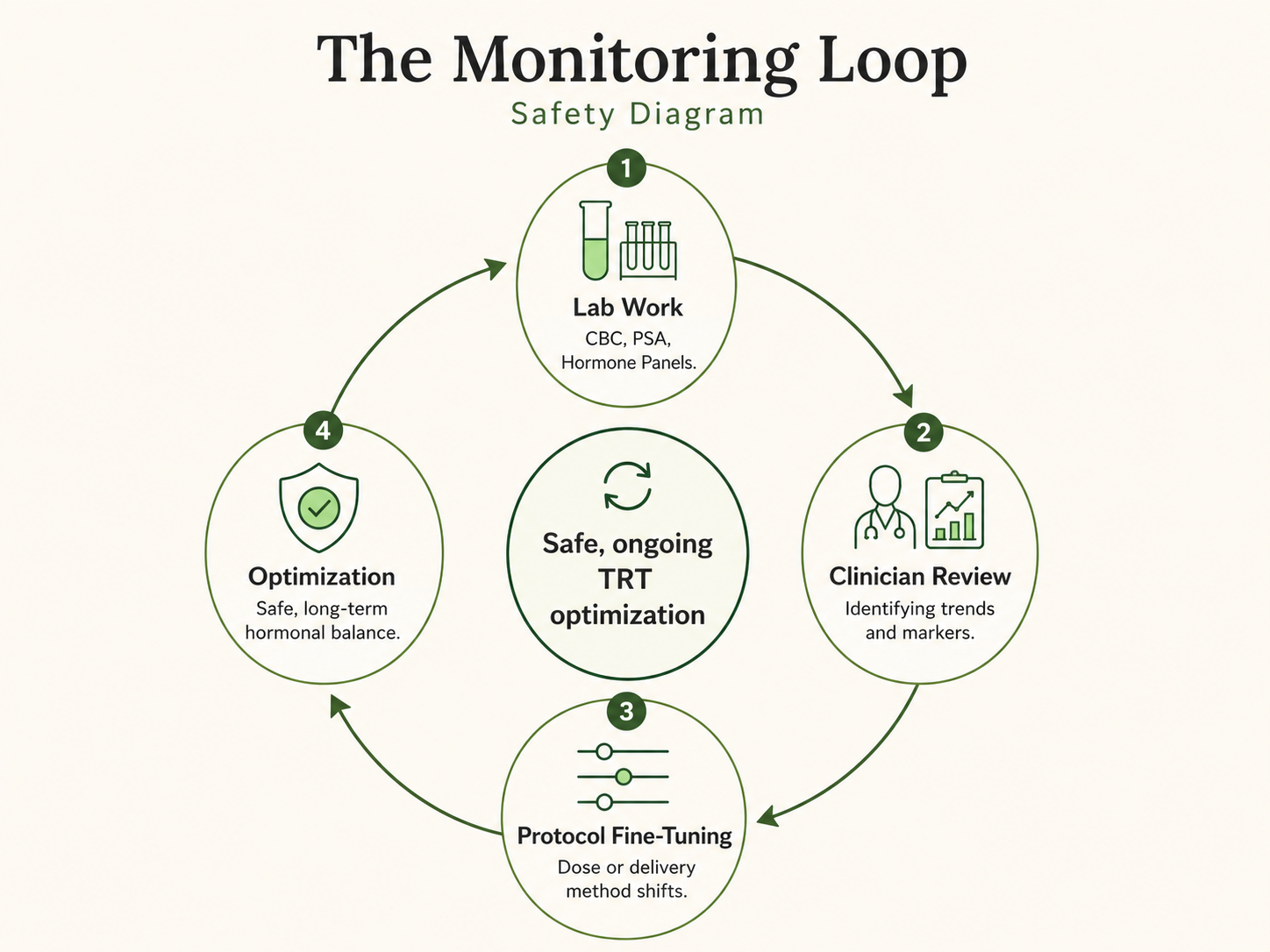
Your blood tests tell the story your symptoms cannot. Total testosterone, estrogen levels, sex hormone binding globulin, red blood cell count, hematocrit, PSA, and liver markers all require regular monitoring throughout therapy. The frequency of lab results review depends on your delivery methods and your healthcare provider's protocol, but most men require blood tests at 3 months and 6 months in the first year, and at least annually thereafter.
Estrogen levels matter particularly. Testosterone converts to oestrogen through aromatisation, and if your oestrogen rises too high, you may experience water retention, mood changes, and reduced libido, which are the same symptoms you started TRT to resolve. Fine tuning your dose or delivery method addresses this before it becomes a problem.
Red Blood Cell Count and the Risk You Cannot Feel
Elevated red blood cell count is the most common dose-limiting effect of testosterone therapy, and it is one you cannot feel until it becomes a problem. A retrospective study in the Journal of Urology found that erythrocytosis developed in 20.1% of hypogonadal men on testosterone therapy at a median follow-up of 7 months, with injectable testosterone associated with a higher rate than topical gels. A long-term cohort study of 1,073 individuals on testosterone therapy, with up to 20 years of follow-up, published in the Journal of Clinical Endocrinology and Metabolism, found that hematocrit increased most significantly in the first year, rising from a mean of 0.39 L/L at baseline to 0.45 L/L after 12 months, with the probability of erythrocytosis continuing to increase over time (10% at 1 year, 38% at 10 years). Elevated hematocrit thickens your blood, raises blood pressure, and increases the risk of clotting events. This is why your blood tests are not a formality. They are what keeps you safe.
If your hematocrit climbs above threshold, your provider may reduce your dose, switch your delivery method, or temporarily pause therapy. These are standard responses, not treatment failures.
Subtle Changes You Might Miss But Shouldn't
Not all of TRT's effects arrive with fanfare. Some of the most meaningful changes come quietly, and you may not notice them until you compare yourself to where you were six months ago.
Sleep Quality
Poor sleep is both a cause and a consequence of low testosterone. As your hormone levels stabilise, many TRT patients report that their sleep quality improves, that they wake feeling more rested, and that the mental heaviness of the morning eases. This is not a guaranteed outcome, and men with untreated sleep apnea should know that testosterone therapy can worsen it. If your sleep worsens after starting TRT, raise this with your healthcare provider immediately.
Skin, Hair, and Subtle Physical Shifts
Testosterone influences skin thickness and sebum production. You may notice changes in skin texture, increased oiliness, or acne, particularly in the early months of treatment. Hair loss is a valid concern for younger men with a genetic predisposition, as testosterone can accelerate androgenetic alopecia. These effects are dose-dependent and vary widely across individuals.
Psychological Factors and Well Being
Well being on TRT is not purely physiological. How you feel about your progress, whether your expectations match your experience, and whether your daily life supports the treatment all make a difference. Men who start TRT while also addressing sleep quality, physical activity, stress, a balanced diet, and underlying health issues consistently report better outcomes than those who rely on testosterone alone. TRT creates the conditions. The rest is still yours to build.
What Ongoing Support Looks Like and Why Stopping TRT Has Consequences
TRT is not a treatment you pick up and put down casually. Stopping TRT without medical guidance allows your testosterone levels to drop, often below where they started, while your natural testosterone production restores itself over weeks to months.
When you stop therapy, you may experience a return of common symptoms including low energy, reduced libido, mood changes, and brain fog. If your natural production has been suppressed for a long period, restoration may be slow. Always discuss stopping TRT with your healthcare provider and follow a managed plan rather than stopping abruptly.
You should also know what would make you a candidate to avoid TRT or pause it. These include rising PSA levels that suggest prostate cancer risk, hematocrit above threshold, untreated or worsening sleep apnea, a recent heart attack, uncontrolled blood pressure, or a confirmed prostate cancer diagnosis. None of these are reasons to avoid asking questions. They are reasons to make sure your ongoing monitoring is thorough.
Some providers use off-label treatments such as clomiphene citrate or enclomiphene to help stimulate natural testosterone production during the recovery period after stopping TRT. Discuss this option with your healthcare provider if recovery of natural production is a priority.
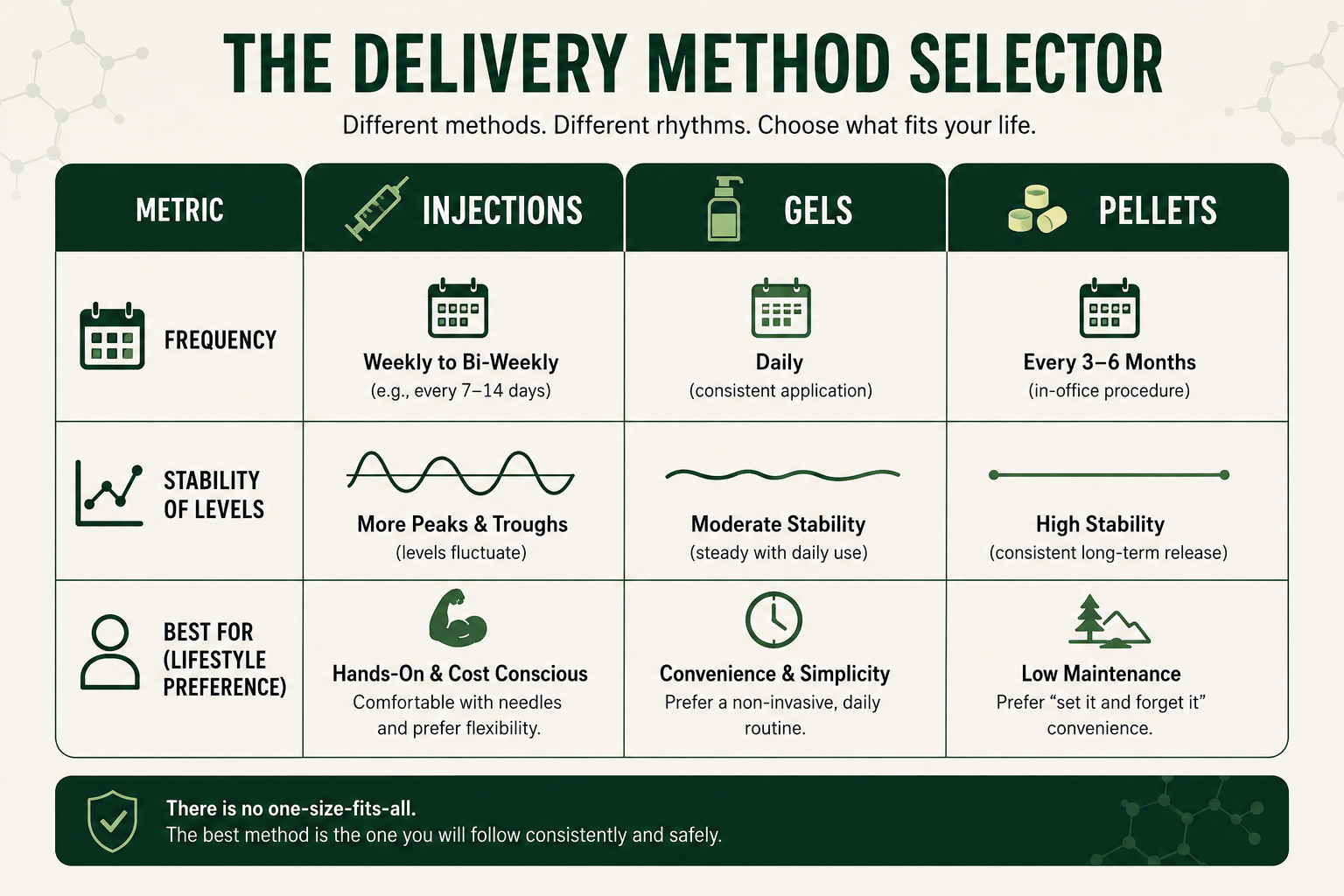
Delivery Methods: What You Are Taking and What It Changes
The delivery method you and your healthcare provider choose affects both your results and your experience on therapy. Each option has a distinct profile.
| Delivery Method | Typical Frequency | Notes |
| Weekly injections | Once weekly | Most common; stable levels with regular dosing; higher hematocrit risk than gels |
| Testosterone gel | Daily application | Steady hormone levels; skin transfer risk to partners; lower erythrocytosis risk |
| Long-acting injections | Every 10 to 12 weeks | High convenience; less fine tuning flexibility if issues arise |
| Subcutaneous pellets | Every 3 to 6 months | Longest acting; requires minor procedure; limited dose adjustment mid-cycle |
The delivery method does not change the fundamental effects of testosterone replacement, but it does influence how consistently your hormone levels stay within range and how easily your provider can adjust your dose if fine tuning is needed.
Frequently Asked Questions
How quickly will I feel different after starting TRT?
Some men notice mood and energy shifts within two to four weeks. Sexual interest can improve by week six. Erectile function and body composition changes typically take three to six months. Do not judge the therapy by what you feel in the first two weeks.
Will TRT make me gain muscle without training?
TRT creates a hormonal environment that supports lean muscle mass growth and reduced fat, but it does not replace resistance training. The research shows the greatest body composition benefits when TRT is combined with consistent physical activity and a balanced diet.
What blood tests do I need while on TRT?
Your healthcare provider will typically monitor total testosterone, estrogen levels, sex hormone binding globulin, red blood cell count, hematocrit, PSA, blood pressure, and liver markers. Most providers schedule blood tests at 3 months and 6 months in year one, then annually.
Is it normal to feel worse before feeling better on TRT?
Some men experience water retention, minor acne, or mood fluctuations in the early weeks as hormone levels adjust. These often settle as your body reaches a stable new baseline. If symptoms persist or worsen, contact your healthcare provider rather than adjusting your dose yourself.
Can I stop TRT if I change my mind?
Yes, but stopping TRT should be managed with your healthcare provider. Your natural testosterone production will have been suppressed and needs time to recover. Stopping abruptly can cause a temporary drop in hormone levels and a return of low testosterone symptoms before your body restores its own production.
Does TRT cause prostate cancer?
Current evidence does not support TRT as a cause of prostate cancer. It does raise PSA modestly, which is why ongoing PSA monitoring is required throughout treatment. Men with existing or suspected prostate cancer are not appropriate candidates for TRT.
How long do I need to stay on TRT?
TRT for confirmed male hypogonadism is typically a long-term treatment. The underlying cause of your testosterone deficiency does not resolve itself. If you stop therapy, your testosterone levels will return to where they were before treatment. Some men with secondary hypogonadism caused by a treatable underlying cause may be able to address that cause and restore natural testosterone production.
Conclusion
Starting TRT is a decision that deserves realistic expectations, not a highlight reel. Your body responds to testosterone replacement on its own timeline, and that timeline does not always match what you hoped for when you started.
The research is clear on a few things: sexual interest tends to shift earlier than erectile function, energy and mental clarity often move before physical changes, and body composition improvements take months, not weeks, and are meaningfully supported by consistent training and good sleep. The men who do best on TRT are the ones who also take their blood tests seriously, communicate changes to their healthcare provider, and do not stop therapy prematurely because they expect faster results.
If you are considering starting TRT or are early in your treatment, the most important thing you can do is build an honest relationship with your provider, keep your lab monitoring consistent, and give your body the time it needs to find its new baseline. The life changing outcomes some men describe are real. They are also the result of patience, monitoring, and doing the work alongside the treatment, not instead of it.
Disclaimer
This content is for educational purposes only and does not replace medical advice. Testosterone therapy and hormone-related health decisions should be guided by a licensed healthcare provider.
References
Hackett G, Cole N, Saghir A, Jones P, Strange RC, Ramachandran S. Testosterone replacement therapy: improved sexual desire and erectile function in men with type 2 diabetes following a 30-week randomized placebo-controlled study. Andrology. 2017;5(5):905-913. doi:10.1111/andr.12399. PMID: 28771964. https://pubmed.ncbi.nlm.nih.gov/28771964/
Yassin AA, Saad F. Improvement of sexual function in men with late-onset hypogonadism treated with testosterone only. J Sex Med. 2007;4(2):497-501. doi:10.1111/j.1743-6109.2007.00442.x. PMID: 17367445. https://pubmed.ncbi.nlm.nih.gov/17367445/
Aversa A, Morgentaler A. The practical management of testosterone deficiency in men. Nat Rev Urol. 2015;12(11):641-50. doi:10.1038/nrurol.2015.238. PMID: 26458755. https://pubmed.ncbi.nlm.nih.gov/26458755/
Wang C, Swerdloff RS, Iranmanesh A, et al. Transdermal testosterone gel improves sexual function, mood, muscle strength, and body composition parameters in hypogonadal men. J Clin Endocrinol Metab. 2000;85(8):2839-53. doi:10.1210/jcem.85.8.6747. PMID: 10946892. https://pubmed.ncbi.nlm.nih.gov/10946892/
Ng Tang Fui M, Prendergast LA, Dupuis P, et al. Effects of testosterone treatment on body fat and lean mass in obese men on a hypocaloric diet: a randomised controlled trial. BMC Med. 2016;14(1):153. doi:10.1186/s12916-016-0700-9. PMID: 27716209. https://pubmed.ncbi.nlm.nih.gov/27716209/
Aghazadeh M, Pastuszak AW, Johnson WG, et al. Elevated dihydrotestosterone is associated with testosterone induced erythrocytosis. J Urol. 2015;194(1):160-5. doi:10.1016/j.juro.2015.01.038. PMID: 25596360. https://pubmed.ncbi.nlm.nih.gov/25596360/
Madsen MC, van Dijk D, Wiepjes CM, et al. Erythrocytosis in a large cohort of trans men using testosterone: a long-term follow-up study on prevalence, determinants, and exposure years. J Clin Endocrinol Metab. 2021;106(6):1710-1717. doi:10.1210/clinem/dgab089. PMID: 33599731. https://pubmed.ncbi.nlm.nih.gov/33599731/