
The answer is not as simple as it seems. The right one between subcutaneous vs intramuscular testosterone injections depends on personal preference. Many men who are undergoing testosterone replacement therapies are unaware of the choice they have. The choice is between intramuscular and subcutaneous injectable testosterone.
Deciding the right choice amplifies the chances of success of your testosterone treatment. The wrong choice may lead to more side effects or hormone swings. Intramuscular and subcutaneous injections both work, but they deliver testosterone to your body differently, with different risk profiles.
This blog explains everything you need to know to have an informed conversation with your doctor about which method fits you best. Learn more!
Disclaimer: This blog is for educational purposes only and does not constitute any medical advice. Always consult a healthcare professional before starting, changing, or stopping your TRT treatment.
Quick Read: Intramuscular vs Subcutaneous Testosterone
| Feature | IM Injection | SubQ Injection |
| Injection Depth | Deep into the muscle layer | Just under the skin into fat tissue |
| Absorption Speed | Faster absorption into the bloodstream | Slower, more gradual absorption |
| Hormone Stability | Can create higher peaks | More stable daily hormone levels |
| Self Injection Case | More difficult to perform on yourself | Easier for self administration |
| Needle Size | 1-1.5 inches long | ⅝ inches or 25–27 gauge |
| Hematocrit Impact | Lower levels post-therapy | Higher levels post-therapy |
| Typical Frequency | Weekly or more often | Weekly to every two weeks |
| Max Volume Per Site | 0.5 mL | 1-3 mL |
What are the Main Injection Routes For Testosterone Treatment?
Intramuscular (IM) and Subcutaneous (SubQ) are the two primary routes for testosterone therapy. Here is the detailed explanation of these two routes:
Intramuscular (IM)
As the name indicates, Intramuscular injections deliver testosterone directly to the large muscle tissues. It has been the commonly practiced method for hypogonadal men for over eight decades. Since the development of testosterone esters, such as testosterone enanthate and testosterone cypionate, IM has been the default method for testosterone treatment.
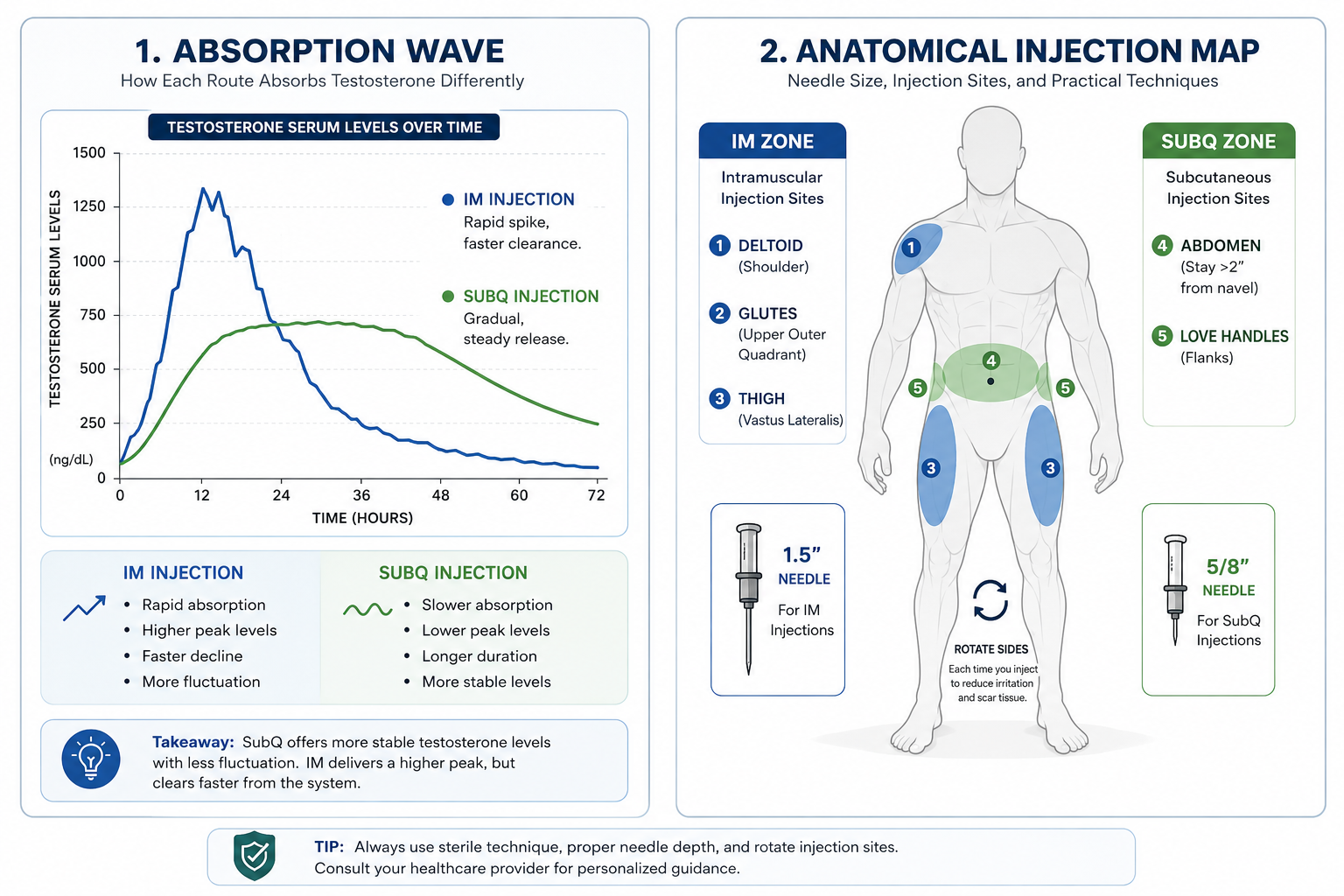
The common injection sites are upper outer gluteus (buttocks), outer thigh (vastus lateralis), and deltoid (shoulder).
The testosterone injection for IM administration is between 22-25 gauge or 1-1.5 inches long. IM injections must be administered at a 90-degree angle.
Subcutaneous (SubQ)
In the subcutaneous (SubQ) method, testosterone injection is placed into fatty tissue (hypodermis) just below the skin. This method uses very thin needles, typically ⅝ inches or 25-27 gauge. Some testosterone injections (testosterone cypionate and testosterone enanthate) can be administered through this method in clinical treatment.
Since 2010, the SubQ method has gained traction and is now widely used around the world in TRT treatment. The first FDA-approved SubQ testosterone injection was Xyosted in 2018. This method also has its pros and cons, and a healthcare professional is the one to decide which injection method best suits you.
Needle Size, Injection Sites, and Practical Techniques
The tools and the injection sites on your body are very different for SubQ vs IM testosterone. The Journal of Clinical Endocrinology and Metabolism explains size, injection sites, and practical techniques in detail:
IM Needle Specs:
An IM testosterone injection needs a needle long enough to go through the skin and fat to reach the muscle. This is often 1 to 1.5 inches long. The gauge (needle thickness) is usually between 22 and 25. The oil the testosterone is mixed with can be thick, so it needs a wider needle to push it through.
SubQ Needle Specs:
A subcutaneous testosterone injection uses a much smaller, shorter needle. The typical length is only 5/8 to 1/2 inch. The gauge is very thin, usually 25-27. This is the smallest needle you can use for this medicine. Patients may feel less fear and pain with this small needle.
IM Injection Sites:
- The ventrogluteal site (the hip muscle).
- The vastus lateralis muscle (the outer thigh).
- The dorsogluteal site (the upper outer buttock).
Research trials suggest that the thigh and buttock are common sites, but the ventrogluteal site is often the safest choice because it avoids the sciatic nerve (biggest nerve in the body).
Subcutaneous Injection Sites:
- The abdomen, making sure you stay at least two inches away from your belly button.
- The tops of the thighs.
- The love handle area (Sides of your waist).
Site Rotation Importance:
You must change your injection spot each time. This is called site rotation. If you inject in the same small spot, you can build up scar tissue under the skin. This scar tissue can make each injection hurt more.
The medicine may also not absorb as well from a scarred area. Use a simple map. Inject on the left side one day, then the right side the next. Rotating sites keeps your tissue healthy for years of testosterone therapy.
Practical Technique for Self-Injection:
For IM Testosterone Injection:
- The first step is to wash your hands thoroughly.
- Then lay out all your equipment on a clean and flat surface.
- Use an 18-gauge filter needle to pull out medication from the vial.
- Once the syringe is full, replace the filter needle.
- Replace the filter needle with an injection needle, which is 22-25 gauge or 1-1.5 inches.
- Gently push the plunger until a small drop appears at the tip.
- Wipe the injection site with an alcohol swab, then let it dry completely.
- Stretch the skin tight over the site, and do not pinch it.
- Insert the needle straight in at a 90-degree angle using one firm, smooth motion.
- Push the plunger slowly to inject the medication.
- Pull the needle out at the same angle it went in.
- Press gently on the area with an alcohol swab.
- Dispose of the used needle safely in a sharps container.
For SubQ Testosterone Injection:
- Wash your hands and prepare your supplies.
- Draw the medication by using an 18-gauge filter needle
- Once it is full, replace it with a 25-27 gauge injection needle.
- Gently push the plunger until a small drop appears at the tip.
- Sterilize the injection with an alcohol swab.
- Pinch a fold of fatty tissue between your thumb and index finger.
- Insert the needle into the center of the fold at a 45-degree angle.
- Inject slowly and steadily.
- Gently remove the needle the same way at a 45-degree angle.
- Apply gentle pressure and dispose of the needle.
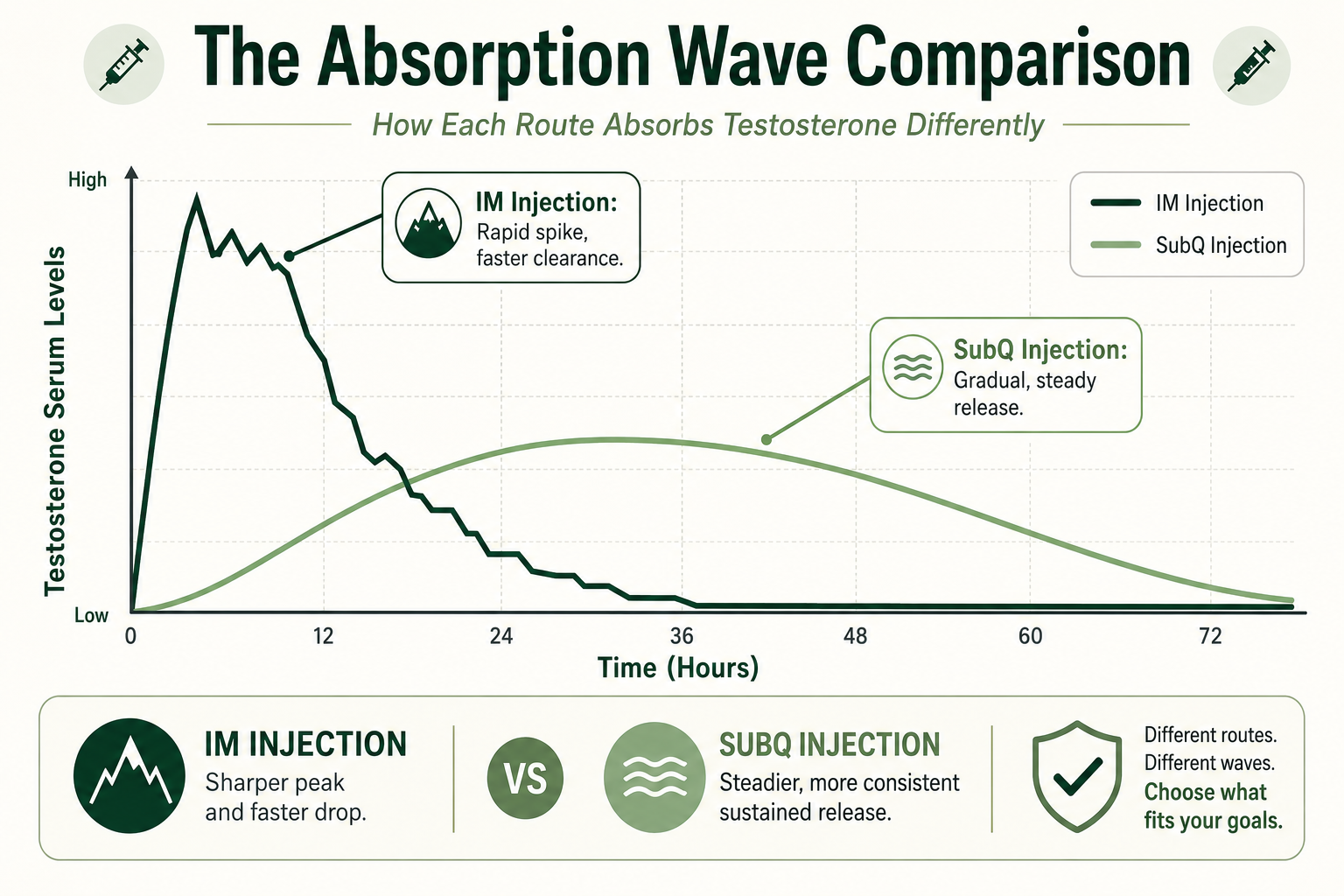
How Each Route Absorbs Testosterone Differently?
Understanding why IM and SubQ produce different results requires a brief look at what happens after testosterone injection. The Journal of Clinical Endocrinology and Metabolism explains how medication is absorbed after entering the body. Have a look at it!
Absorption Mechanism of Intramuscular (IM) Route:
Muscles are rich with blood vessels. When the testosterone oil depot is placed inside a muscle, it sits next to a huge network of capillaries. This allows the medicine to enter the bloodstream more quickly.
According to research investigations in the Journal of Clinical Endocrinology & Metabolism, the IM route can lead to a rapid peak in serum testosterone levels within 24 to 48 hours after the shot.
But keep in mind that each muscle tissue has different blood flow rates and this flow can affect the absorption rate of testosterone injection.
The body then clears the hormone faster, which can sometimes create a hormonal “roller coaster” with ups and downs.
Absorption Mechanism of Subcutaneous (SubQ Route):
Fat tissue has far fewer blood vessels than muscle. When the testosterone oil depot is injected into the fat layer, it sits away from a dense blood supply. The body absorbs the medicine much more slowly.
The same research investigations show that SubQ injections result in a slower, more gradual release of testosterone into the system. This helps avoid the very sharp peak you see with IM shots. The steadier absorption mirrors the body’s natural daily hormone rhythm more closely.
Is Subcutaneous as Effective as Intramuscular?
Yes, for many patients, it is. Clinical studies directly comparing SubQ vs IM testosterone show they are both effective. Various studies have found that subcutaneous testosterone therapy was as effective as the intramuscular method at achieving normal total testosterone levels.
A 2015 phase II study published in the Journal of Sexual Medicine evaluated subcutaneous testosterone enanthate in 39 hypogonadal men. The study found that men receiving 50 mg or 100 mg weekly SubQ doses achieved steady state testosterone levels compared to those men on standard 200 mg IM injections.
The American Journal of Health-System Pharmacy also confirmed that SubQ is equally effective as an IM injection route. Based on these research studies, it has proven that the SubQ injection method is as useful and effective as IM injection method. The SubQ route delivers the same results in a more steady way. It is not a lesser or a compromised method.
Side Effects Mechanism: Where These Routes Diverge
Hematocrit (HCT) and Estradiol (E2) Elevation:
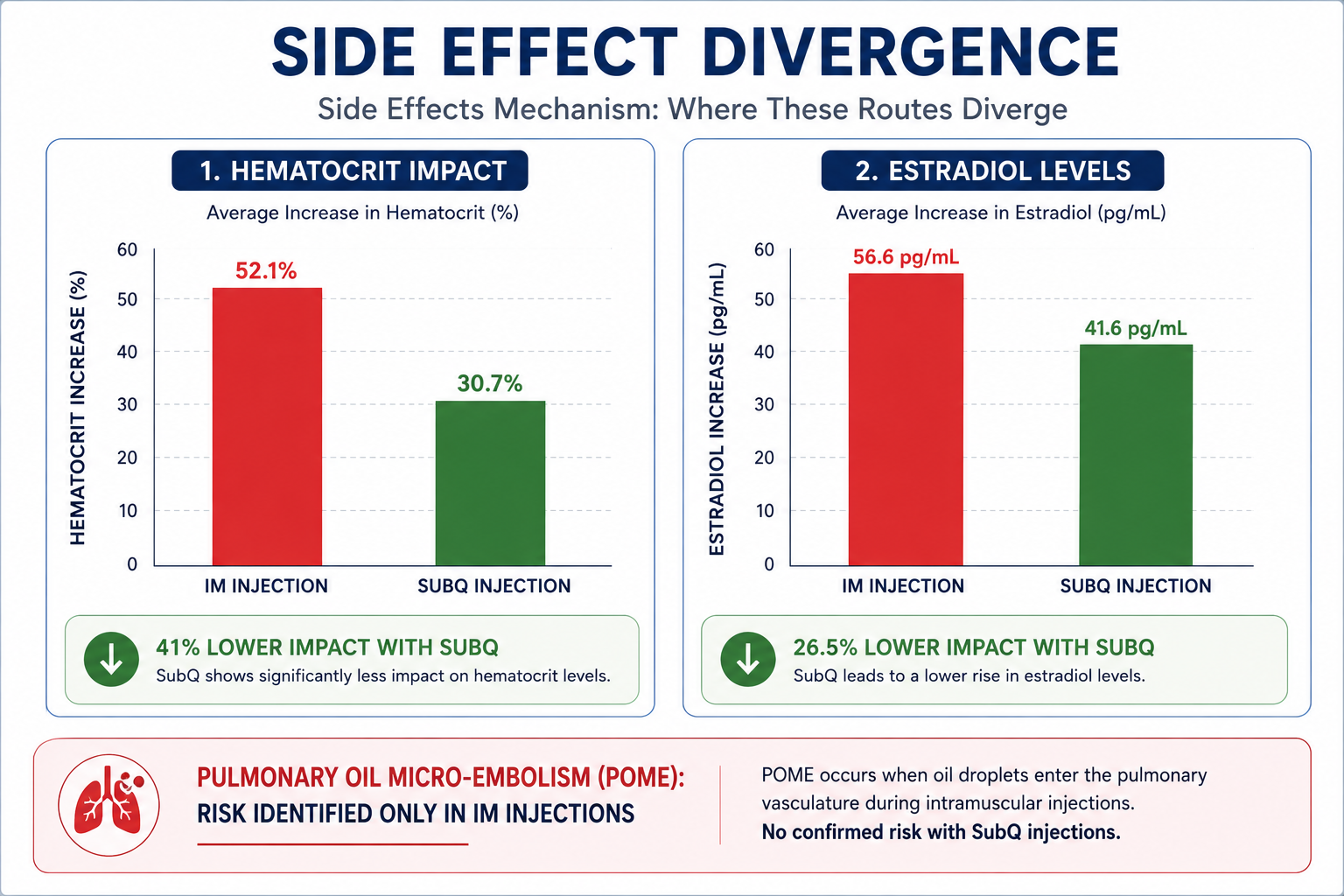
Research studies suggest that SubQ has a lower impact on hematocrit and E2 elevation in hypogonadal men compared to IM injection. A study published in 2022 in The Journal of Urology compared 234 men treated with either SubQ enanthate or IM testosterone cypionate. The study found the following results:
- SubQ patients had 41% lower post-therapy hematocrit than IM patients.
- SubQ patients had 26.5% lower Estradiol (E2) levels compared to IM patients.
- No significant differences in PSA elevation were seen.
Injection Site Reaction:
SubQ testosterone injections can create mild local reactions, such as redness or small nodules, if the same site is used repeatedly. On the other hand, IM testosterone injections can cause muscle soreness, bruising, and hematoma at the injection site.
Pulmonary Oil Micro-Embolism (POME):
The Pulmonary Oil Micro-Embolism (POME) is only seen in the IM injection route in published literature. When a small oil drop enters the bloodstream during IM injection, it can cause respiratory problems, coughing, or dizziness. This health issue is not associated with the SubQ testosterone injection route.
How Often Should You Inject with Each Method: Injection Frequency
Injection frequency for IM and SubQ differ from each other. Here is a detailed overview:
Intramuscular Injection Frequency:
Because the peak is high and the clearance is faster with IM shots, the standard schedule may be once every two to three weeks. However, this schedule can lead to large mood and energy swings. A better modern approach, according to research studies, is to inject a smaller IM dose (50mg or 100mg) once every one to two weeks to create more stable blood levels.
Subcutaneous Injection Frequency:
The most common schedule for a subcutaneous testosterone injection is once or twice a week. This is often done with testosterone cypionate subcutaneous injections. The small needle and easy pinch method make frequent injections much less of a burden. This schedule keeps hormone levels in a very stable, narrow range.
Common SubQ Dosing Schedule:
- Once weekly (Standard)
- Twice weekly (split dose for smoother levels)
- Daily micro dose (Most stable, lowest peak)
Who Should Choose Subcutaneous and Who Should Choose Intramuscular Injections?
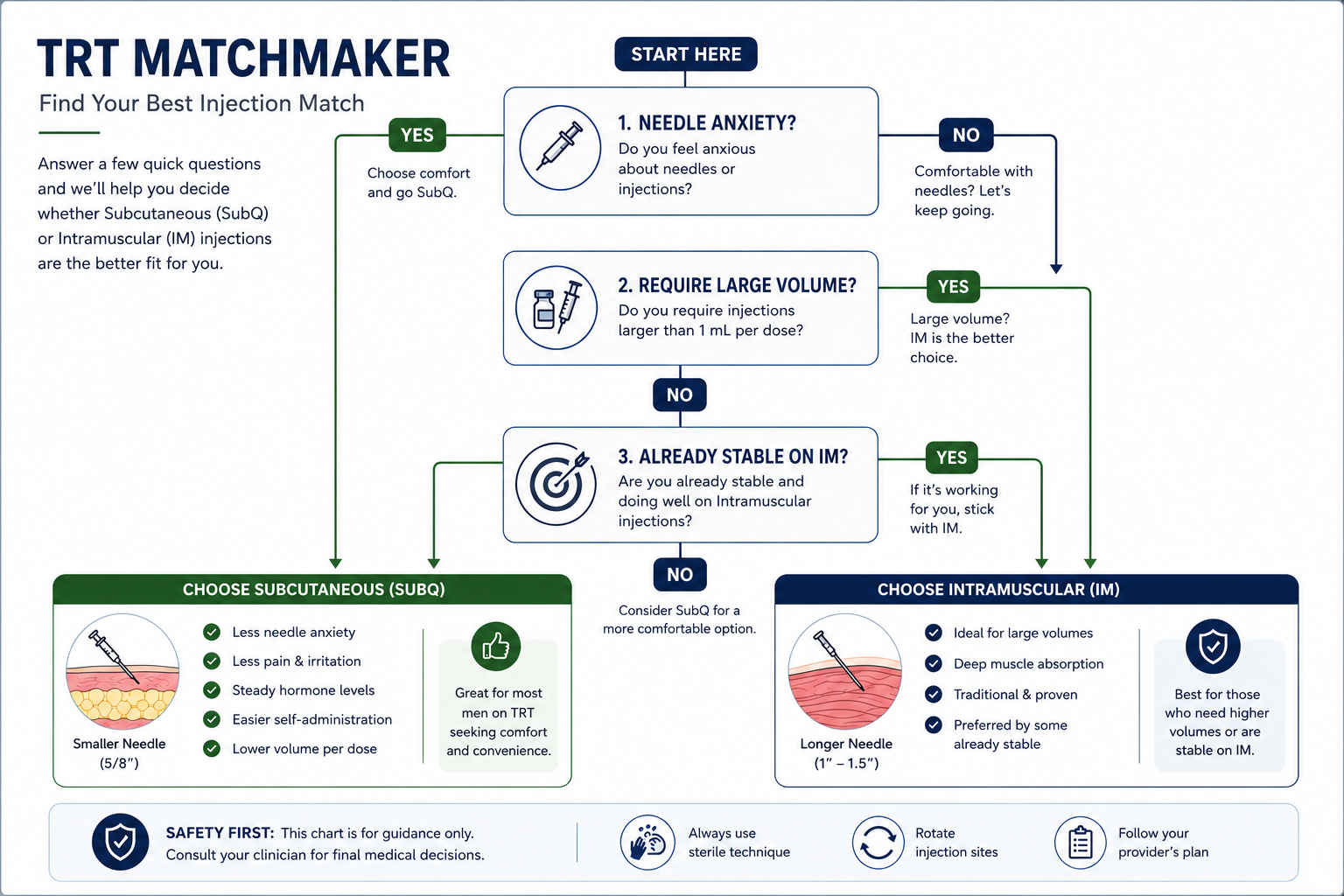
Consider SubQ If You Have:
- Elevated Hematocrit (50-52%) on IM TRT
- Experienced high E2 and related symptoms (water retention or mood changes) in IM TRT
- Struggled to self-inject your glutes
- Needle anxiety (SubQ needles are very thin)
- Want to inject more frequently
- Pain anxiety (SubQ causes less pain)
Consider IM If You Have:
- Require a large single-injection volume
- Prefer less frequent injections (bi-weekly)
- Have very low body fat with minimal subcutaneous tissues
- Are already well-controlled on IM
- Are receiving testosterone undecanoate (IM route is preferred)
What to Track Regardless of Which Injection Method You Use?
Monitor the following lab-results:
- Total testosterone (trough level)
- Free testosterone levels
- Estradiol (E2) level
- Hematocrit and hemoglobin in your body
- PSA (prostate specific antigen) levels
- LH and FSH levels
Important Note:
- Always test your testosterone levels early in the morning or day before your next injection.
- Stable patients must do annual monitoring, and new patients 3-4 months after starting.
Common Mistakes Men Make With Testosterone Injection
Even smart men make simple errors that can defeat the purpose of testosterone therapy.
- Injecting Too Infrequently: Injecting too frequently can cause huge hormonal swings.
- Not Rotating Sites: Using the same spot over and over creates scar tissue and uneven absorption.
- Injecting Too Fast: You should push the plunger very slowly. The oil needs time to spread into the tissue.
- Using Too Large a Needle for SubQ: A long, thick needle meant for IM is not for SubQ use. It would inject the medicine too deep, missing the fat layer.
- Ignoring the Expiration Date: Using old medicine is dangerous. A broken-down, expired vial may not work, and the chemical change could cause a reaction.
Frequently Asked Questions (FAQs)
Which has faster absorption: IM or SubQ?
Intramuscular testosterone injection has a faster absorption rate compared to SubQ injection. Because muscle tissue has a richer blood supply than subcutaneous fat.
Is Intramuscular more painful than subcutaneous?
Intramuscular injections are slightly more painful than subcutaneous injections due to deeper needle penetration. The SubQ needle is thin and thus causes less pain compared to the IM needle.
Can you take TRT subcutaneously?
Yes, you can take testosterone replacement therapy subcutaneously with smaller and frequent doses. Many studies support that SubQ testosterone is as effective as IM testosterone treatment.
What is better for TRT: SubQ or IM?
Neither is universally better. IM testosterone provides faster results with higher peaks, whereas SubQ provides stable and slower peaks. The choice depends on your personal preference, pain tolerance level, and healthcare recommendations.
What is the easiest spot to inject testosterone?
The gluteus medius (upper outer of the buttock) is the easiest spot to inject IM testosterone, whereas the abdomen is easiest for SubQ. These sites cause minimal pain.
What are the benefits of SubQ testosterone?
SubQ testosterone uses smaller needles, which causes less pain and minimizes the chances of scars at the injection site. It also provides more stable hormone levels with lower risks.
What happens if you inject testosterone into fat instead of muscle?
Injecting testosterone into fat instead of muscle tissues slows absorption rate. You will still absorb testosterone but at a slower rate with a steady and stable peak.



