If you are on testosterone replacement therapy, getting your labs done is not just a formality. It is the mechanism through which your provider knows your treatment is working and that you are not developing serious side effects. That is the direct answer to why monitoring matters.
You may have started TRT because of confirmed low testosterone and symptoms like fatigue, reduced drive, or changes in body composition. The treatment itself carries real benefits for men with clinically confirmed testosterone deficiency. But testosterone therapy also shifts several systems in your body, including your red blood cell production, your prostate, your cardiovascular risk profile, and your hormone balance, in ways that need to be tracked over time.
Understanding which labs get ordered, when they are drawn, and what the results mean puts you in a better position to have informed conversations with your provider. It also helps you recognize when something in your numbers is worth discussing rather than waiting until your next scheduled appointment.
This article covers the baseline labs required before starting testosterone therapy, the ongoing monitoring schedule, what each test is measuring and why it matters, and how your provider uses those results to make dose adjustments or flag concerns.
Why Monitoring Is Non-Negotiable on TRT
Testosterone therapy is not a set-and-forget treatment. Monitoring is built into standard clinical practice because the therapy directly changes your physiology in ways that can accumulate risk over time without producing obvious symptoms.
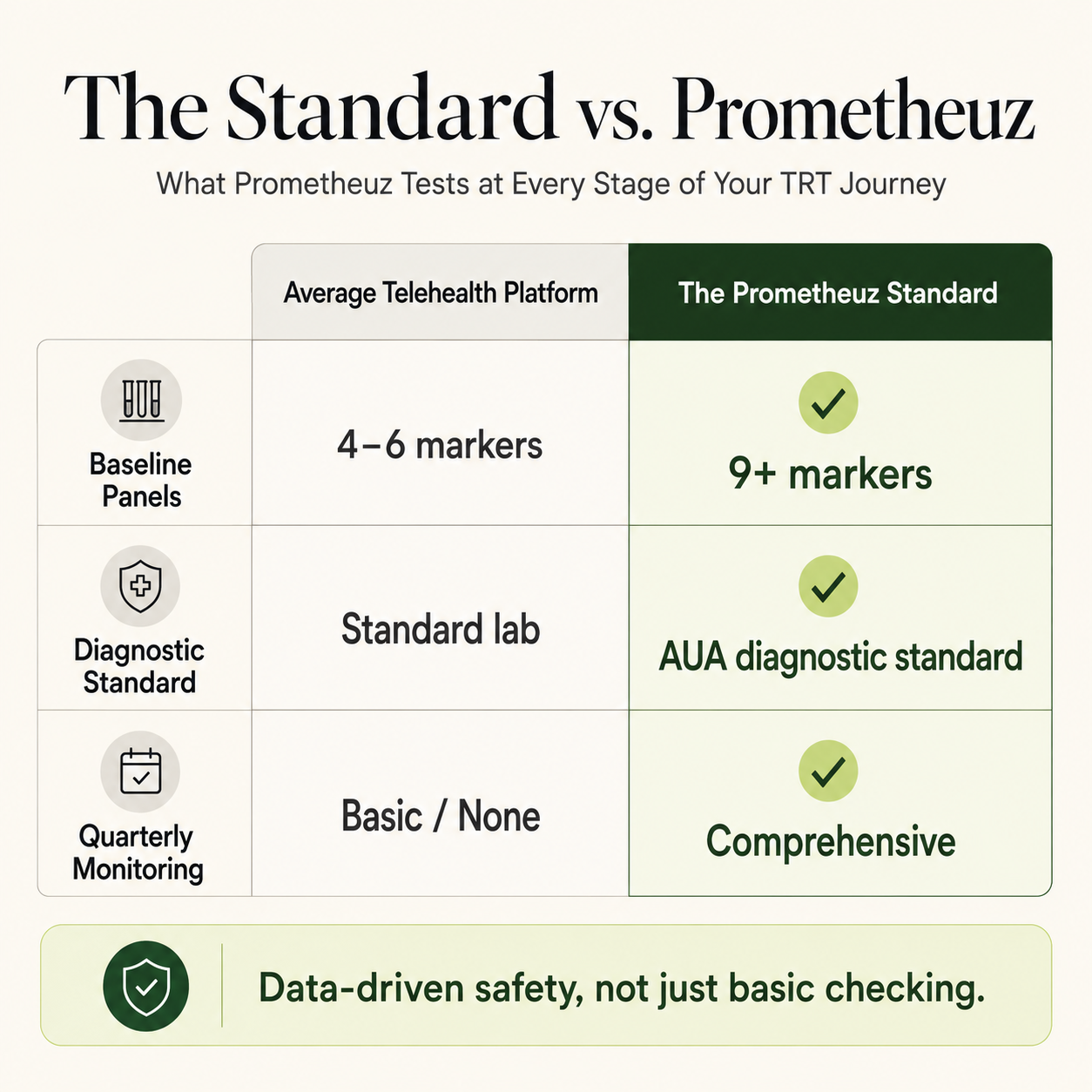
The Endocrine Society clinical practice guidelines, one of the most referenced frameworks for managing testosterone deficiency syndrome, specify monitoring at defined intervals before and during treatment. A review published in Acta Medica Indonesiana summarizing clinical practice guidelines for hypogonadism noted that the Endocrine Society recommends testosterone levels between 400 and 700 ng/dL one week after administering testosterone enanthate or cypionate, with ongoing monitoring of hematocrit, PSA, and clinical symptoms at 3, 6, and 12 months and annually thereafter.
You might find it inconvenient to schedule blood draws every few months. But consider what those draws are actually catching: changes in your red blood cell count that increase clotting risk, PSA shifts that may signal prostate changes, and testosterone levels that tell your provider whether your dose is landing in a therapeutic range or overshooting it. Missing a draw does not mean nothing is happening. It means you are not seeing what is happening.
Labs You Need Before Starting Testosterone Therapy
Before your provider initiates testosterone therapy, a baseline set of labs is required. These are not just precautionary. They establish the reference points everything else is compared against.
Your Testosterone Levels at Baseline
Total testosterone and free testosterone are the starting point. The Endocrine Society defines testosterone deficiency as a serum testosterone below the normal range confirmed on two separate morning blood draws. Morning blood draws matter here because testosterone peaks in the early morning and declines across the day. A single afternoon reading is not sufficient for diagnosis.
Sex hormone binding globulin (SHBG) is measured alongside testosterone because a significant portion of circulating testosterone is bound to this protein and is biologically inactive. High SHBG can make your total testosterone appear adequate even when free testosterone, the fraction that actually acts on tissue, is low. If your provider suspects this pattern, bioavailable testosterone provides additional clarity.
Luteinizing hormone (LH) is drawn to identify where the problem originates. Low testosterone with low LH points to a signaling failure at the pituitary or hypothalamus, which is called secondary hypogonadism. Low testosterone with high LH suggests the testes themselves are not responding, which is called primary hypogonadism. This distinction shapes how your treatment is managed.
Prostate-Specific Antigen
PSA, which stands for prostate-specific antigen, is measured at baseline before you begin treatment. This is a prostate cancer screening step, not an afterthought. Testosterone stimulates prostate tissue, and starting therapy on a man with undetected prostate cancer carries real risk. Men with active or suspected prostate cancer are contraindicated for testosterone therapy. French urology guidelines published in Progres en Urologie list progressive prostate cancer alongside breast cancer and recent cardiovascular events among the contraindications to treatment.
If your baseline PSA is elevated or your provider has clinical concerns, prostate cancer screening must be completed before testosterone therapy begins.
Complete Blood Count
Your complete blood count, also called a CBC, establishes your baseline red blood cell count, hematocrit, and hemoglobin before therapy. These numbers matter because testosterone increases red blood cell production. If your hematocrit is already elevated before you start, your provider needs to know that and factor it into the treatment decision.
Comprehensive Metabolic Panel
Liver and kidney function testing via a comprehensive metabolic panel gives your provider a baseline view of organ health. Testosterone is metabolized by the liver, and while liver toxicity is primarily a concern with oral testosterone formulations, baseline liver enzymes are standard practice before starting any testosterone preparation.
Blood sugar and metabolic markers are also captured here. Men with testosterone deficiency frequently have concurrent metabolic issues including insulin resistance, elevated blood sugar, and poor lipid profiles, and these interact with the treatment response.
The Monitoring Schedule: When to Get Tested
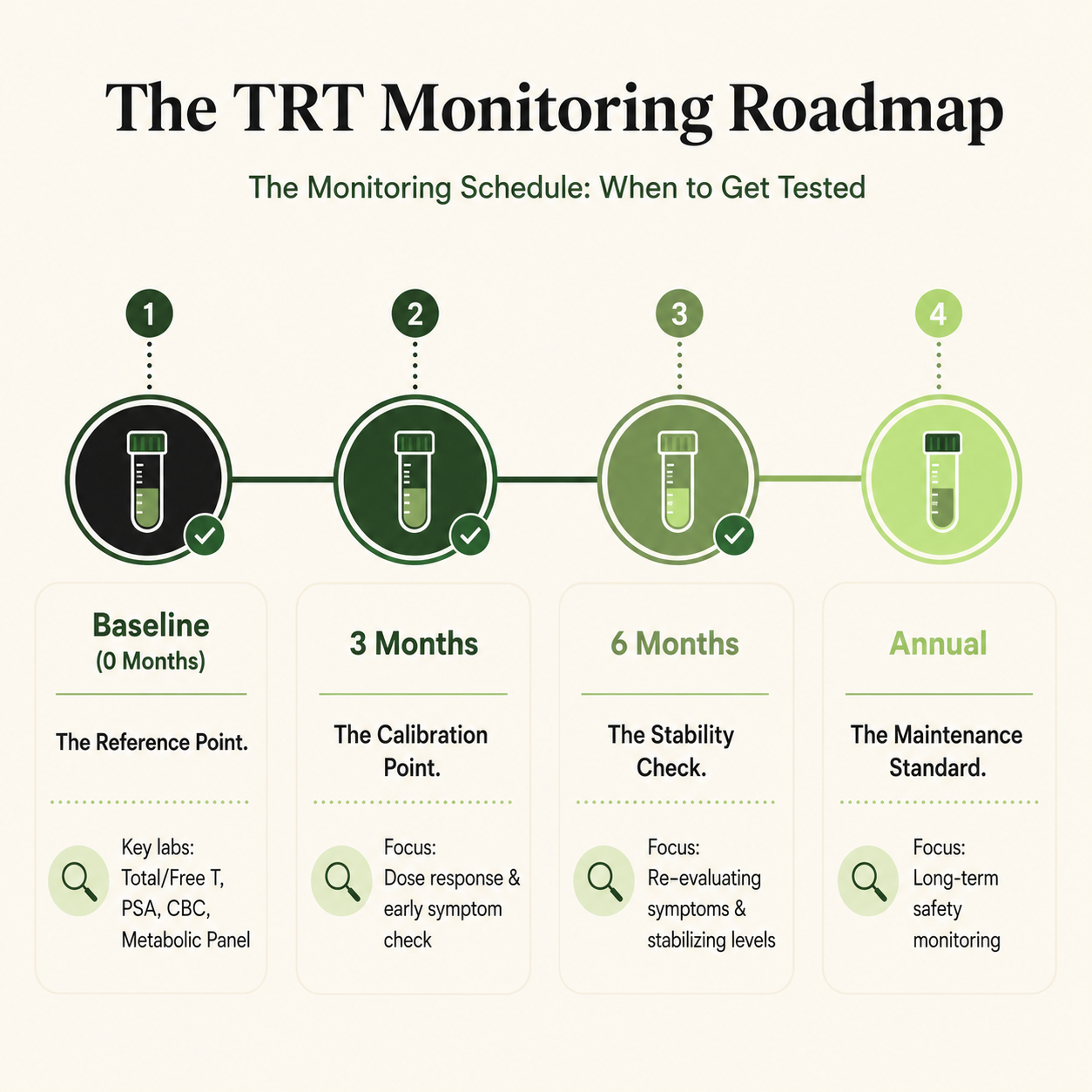
The monitoring schedule follows a defined pattern based on when changes are most likely to occur and when dose adjustments are most often needed.
Starting Testosterone Therapy: The First 3 Months
The period immediately after starting testosterone therapy is the most dynamic. Your body is adjusting to exogenous testosterone, your red blood cell production begins to shift, and your provider needs to confirm that your testosterone levels are landing in a therapeutic range with your specific formulation and dose.
You should expect a blood draw at 3 months after starting treatment. At this point, your provider is checking:
- Total and free testosterone to assess whether your dose is producing target levels
- Hematocrit and hemoglobin to catch early red blood cell elevation
- PSA for any early shift from baseline
- Liver enzymes if indicated by your formulation or baseline findings
If your testosterone levels are outside the target range at 3 months, your provider will adjust the dose before continuing. You should not wait until the 6-month mark if something feels off clinically. Symptoms that change significantly after starting treatment are worth a conversation earlier.
The 6-Month Check
A second draw at 6 months confirms that any dose adjustment from the 3-month visit is working and that your hematocrit trajectory is stable. This is also a natural point to reassess symptoms. If your testosterone levels are now in range but you are not experiencing improvement in the symptoms that led to your diagnosis, that clinical information informs whether the diagnosis and treatment plan are correct.
PSA is checked again at 6 months. The French urology practice guidelines specifically recommend biological monitoring, including total testosterone, PSA, and complete blood count, at 3, 6, and 12 months, and annually thereafter. This cadence is consistent across major clinical guidelines.
Annual Monitoring Once Stable
Once your dose is stable and your labs have been consistent across the first year, annual monitoring becomes the standard rhythm. Your annual labs should include:
- Total and free testosterone
- Complete blood count with hematocrit and hemoglobin
- PSA and digital rectal exam
- Comprehensive metabolic panel
- Liver function if applicable
- Bone density scan every 1 to 2 years for men with confirmed testosterone deficiency, particularly those with low baseline bone mass
You might find annual visits feel routine once your numbers are stable. That routine is the point. It gives your provider the longitudinal data to catch gradual changes before they become clinical problems.
Understanding Each Lab: What It Measures and Why It Matters
Free Testosterone and Total Testosterone
Total testosterone measures all circulating testosterone while free testosterone measures only the biologically active portion your cells can actually use. Both are tracked because your SHBG level determines how much of your total testosterone is available, meaning a normal total number can still mask a low free testosterone. For men on TRT, the target range is generally 400 to 700 ng/dL measured at trough, which is just before your next injection when levels are at their lowest. You want your trough in range, not just your peak.
Hematocrit and Hemoglobin
Testosterone stimulates red blood cell production, which thickens the blood and raises your clotting and cardiovascular risk if levels climb too high. Hematocrit above 54 percent is the clinical threshold where your provider will act, either by reducing your dose, extending your injection interval, or recommending therapeutic phlebotomy. You may feel completely normal when your hematocrit is elevated, which is exactly why this lab cannot be skipped. Research also shows that men with obstructive sleep apnea on TRT are more than twice as likely to develop dangerously elevated red blood cells, so if that applies to you, your provider needs to know.
Prostate-Specific Antigen
PSA is a protein your prostate produces, and because testosterone stimulates prostate tissue, it is monitored throughout your entire time on TRT. A significant rise from your baseline, generally more than 1.4 ng/mL or a rapid increase over a short period, requires investigation before treatment continues. Current evidence does not show that TRT causes prostate cancer in men without pre-existing disease, but it can accelerate growth in cancer that already exists, which is why screening before and during treatment is non-negotiable.
Comprehensive Metabolic Panel and Liver Function
The comprehensive metabolic panel tracks your kidney function, liver enzymes, blood sugar, and electrolytes throughout treatment. Liver enzyme monitoring matters most if you are on oral testosterone, though baseline and periodic checks are standard regardless of your formulation. Because testosterone deficiency is often tied to insulin resistance, your provider will also track blood sugar as testosterone levels improve and metabolic function shifts.
Bone Density
Bone density scanning is recommended for men with confirmed testosterone deficiency, particularly those who have had low testosterone for an extended period before starting treatment. A controlled clinical trial published in JAMA Internal Medicine found that testosterone treatment for one year in older men with low testosterone significantly increased volumetric bone density and estimated bone strength at both the spine and hip compared with placebo. The effect was more pronounced in trabecular bone and more evident in the spine than the hip.
You may not associate testosterone with bone health, since that association is often discussed primarily for women. But men with prolonged testosterone deficiency do lose bone mass, and your provider may recommend a DEXA scan at baseline and every one to two years during treatment depending on your age, deficiency duration, and fracture history.